Download
1 / 26
280 likes | 353 Views
Where are we going wrong ? The story behind unneccessary deaths and suffering. Renée Otter , MD, PhD … . Sequences in oncological care. Treatment A. Early detection. staging. diagnosis. Treatment B. rehabilitation. Palliative care. Patients ’ pathway ( journey ).

E N D
Where are wegoingwrong?The story behindunneccessarydeaths and suffering Renée Otter, MD, PhD…..
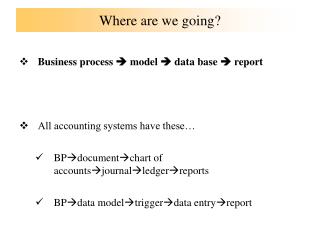
Sequences in oncological care Treatment A Earlydetection staging diagnosis Treatment B rehabilitation Palliative care Patients’ pathway (journey)
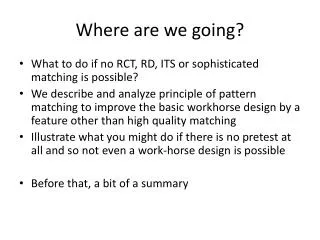
Sequences in oncological care Treatment B Treatment A Earlydetection staging diagnosis Treatment C rehabilitation Palliative care Patients’ pathway (journey)
Sequences in oncological care Treatment B Treatment C Re-staging Treatment A Earlydetection staging diagnosis rehabilitation Palliative care Patients’ pathway (journey)
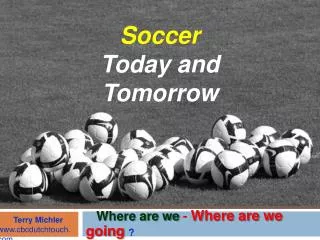
Patients’ pathway (journey) Earlydetection diagnosis staging Treatment A Treatment B rehabilitation
Earlydetection • Reason for this: tackleprecursor situations to cancer or cancer in an early stage as « the earlier the cancer isdetected, the bettersurvival »
Earlydetection • Not all precursor stages of cancer (dysplasia) lead to cancer • If precursorstages of cancer (dysplasia) lead to cancer, the real lead time isunknown (varyfromsomeyears to >20) • overtreatment? Undertreatment!
Earlydetection • Reason for this: tackleprecursor situations to cancer or cancer in an early stage as « the earlier the cancer isdetected, the bettersurvival » • Individual (PSA) • Organised (screening programme) • Participation depends on a.o. the public awareness of symptoms (and the character of the person), the knowledge of the GPs • knowlegde of how to do the tests (based on what?? • by whom • where to go if ever the results are not « within the norms » • The health system shouldstimulate participation and knowledge
Sequences in oncological care Treatment B Treatment A Earlydetection staging diagnosis Treatment C rehabilitation Palliative care Patients’ pathway (journey)
Diagnosis and staging • Once screening or symptoms (rare find by chance) • Diagnosisneeds: • Knowledge on the 150 different types and subtypes of malignancies: Cancer is NOT 1 disease • physicalexamination • Radiology (+ nuclearmedicine) • Pathology • synthesis : diagnosis AND stage • Stage necessary to plan the right treatments
Diagnosis and staging • Where are wegoingwrong • Knowlegde of the GP to whom to refer • Knowledge of the medicalspecialist: if not a cancer specialist (but vice versa istruetoo!!) • Availability of diagnostic equipments ( financial position of a country) AND • trainedradiologists!!! • Trainedpathologists intra – and intervariabilitypanels • Availablility of dedicated MDT ( different disciplines of medicalspecialists) • Knowledge and availability of evidencebased guidelines and staging classifications (TNM)
Diagnosis and staging • Wherecanweget information? • On delay on diagnosis and staging • On minimal imagingtechnics for that cancer • On Quality of the radiologist and pathologist?? • Will this information of any help? To whom? • Sensation and loss of confidence for nothing!! thatswherewe are goingwrong. • Second opinion: isitindependant?!
Sequences in oncological care Treatment B Treatment A Earlydetection staging diagnosis Treatment C rehabilitation Palliative care MDT
Multidisciplinary teams • Who are they: • Combination of diagnosic and treatmentspecialists • Trained • Experienced • Integrated • Sharesresponsabilities in takingdecisionsconcerningtreatment plan
Multidisciplinary teams • Where are wegoingwrong? • Trained?!Are therespecial training programmes, are somespecialisationsrecognisedlikeonco-urologists?! NO EU decisions • Experienced: whatdoesthismean: volume? Outcome? % of complications? What about a small country??what about rare cancers? Variation among EU ishuge • Integratedin a dedicated team : requests trust and confidence!!! • How to measurewhatis right and wrong? Complication rates?? survival?? Patients experiences?? • Financial position of medicalspecialists in a private versus public sector • Who/ whatwill & cantake the decisionsconcerningwhich team isdedicated?!
MedicalTreatment • Where are wegoingwrong? • How to measurewhatis right and wrong? • Are evidencebased guidelines alwaysproviding the right treatmentopportunities for every one?? Individual/personalizedmedicine??? • Availability of new or expensivedrugs? Be careful as drugsonly have a small impact on the survival
No « changes » in stage over 10 years • More stage I breast cancer because of the change of TNM classification • Increase in stage I prostate cancer because of PSA • No change in stage in colon cancers; in rectal cancers less stage I & II because of procedures: endo-echo, MRI, Pet scan • More stage IV lung cancer because of PET scan
Sequences in oncological care Treatment B Treatment A Earlydetection staging diagnosis Treatment C rehabilitation Palliative care Supportive care
Rehabilitation • Support patients to go back to the society • Hugeproblem the more patients become (ex) patients increasesurvivorship • Are thereGLs? Trainedprofessionals?? • No impact on survival but on Quality of life • « LIVING NOT SURVIVING »
From the OECD • Differences in cancer survival • half of it may be explained by the available resources (imaging techniques ,infrastructure, new drugs, NHE) • ¼ by process quality of delivery of care(early detection, access,optimal treatment) • ¼ by governance (NCCP, coordination….) • Where are we going wrong? • Do we treat survival or quality of life?????