Download
1 / 37
440 likes | 1.37k Views
Warfarin counselling. Adrienne Lancaster Anticoagulant Pharmacist Adrienne.lancaster@elht.nhs.uk. East Lancs Hospitals Anticoagulant clinics. 4183 patients registered (Aug 2012) Approx 70,000 patient contacts/ appointments per year Average recall interval 25-30 days

E N D
Warfarin counselling Adrienne Lancaster Anticoagulant Pharmacist Adrienne.lancaster@elht.nhs.uk
East Lancs Hospitals Anticoagulant clinics • 4183 patients registered (Aug 2012) • Approx 70,000 patient contacts/ appointments per year • Average recall interval 25-30 days Where our patients attend for dose advice • Hospital clinics at RBH & BGH • Community Clinics in 10 different locations in PHCC premises throughout district Also home testing and “remote” dosing for housebound patients
GP lead anticoagulant services Darwen Health Centre Parkside Practice Whalley Clitheroe-Castle Group - Pendleside
CHADS2 ScoreBF Gage et al. Validation of clinical classification schemes for predictingstroke. Results from the national registry of atrial fibrillation. JAMA 2001 285: 2864-2870. • This is a simple points system to predict the overall risk of a thrombotic event in a patient with AF • C history of congestive heart failure • H history of hypertension • A age over 75 years • D history of diabetes mellitus • S2 history of stroke or transient ischaemic attack (TIA) • Score one point for each risk and two points for history of stroke/TIA • CHADS2 0 or 1 use CHA2DS2-VASc • CHADS2 ≥ 2 High risk: anticoagulants
CHA2DS2-VAScCHEST 2010 137:263-72 Lipp G,Nieuwlat R, Pisters R et al. Refining clinical risk stratification for prediction of stroke and thromboembolism in atrial fibrillation using a novel risk based approach: the euro heart survey on atrial fibrillation C Congestive heart failure / left ventricular dysfunction score 1 H History hypertension score 1 A2 Age over 75 score 2 D Diabetes mellitus score 1 S2 History or stroke or TIA score 2 V Vascular disease-CAD,MI,PAD score 1 A Age 65-74 score 1 Sc Sex is female score 1 Score 0 Low risk Score 1 Intermediate risk Score 2 or more High risk Score 0 No treatment or aspirin (no treatment preferred) Score 1 Anticoagulant or aspirin consider risk/benefit and HAS-Bled score (Anticoagulant preferred) Score 2 or more: Anticoagulants
HAS-BLED score Hypertension: 1 point for uncontrolled high blood pressure, with a systolic (top number) reading of 160 or higher Abnormal kidney and/or liver function: 1 point for impaired kidney or liver function, and 2 points for both Stroke: 1 point for previous history of stroke, especially deep brain (lacunar) stroke Bleeding: 1 point for previous history of bleeding, anemia or having predisposition to bleeding Labile INR: 1 point for unstable or high INRs, or poor time (less than 60%) in the therapeutic time range Elderly: 1 point for age 65 or older Drugs and/or alcohol: 1 point for taking antiplatelet drugs and 1 point for consuming 8 or more alcoholic drinks per week, or 2 points for both Score 3 or higher is not a contra-indication to anticoagulation but these patients require more care
Warfarin: Adverse effects Haemorrhage- bleeding risk increases with INR >5 Teratogenic GI upset / diarrhoea Liver damage (rare) Skin reactions, hypersensitivity Skin necrosis (rare) more common in protein C deficiency and high loading doses, occurs within days of starting treatment. Alopecia
Monitoring of warfarin International Normalised Ratio Time taken for blood to clot (prothrombin time PT) compared to an international standard Prothrombin time (PT): the time taken for fibrin formation is determined. The result obtained is divided by the geometric mean of normal PTs for a given method. An international sensitivity index (ISI) is then applied to produce an International Normalised Ratio (INR). Prothrombin time, expressed as INR, is used to monitor warfarin because it is sensitive to levels of vitamin K dependant clotting factors 11, V, V11 and X.
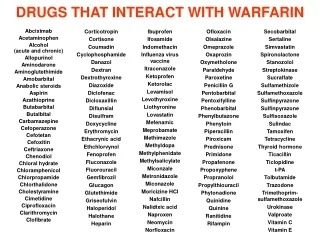
Factors affecting INRDrug interactions Pharmacokinetic Change in plasma concentration of warfarin Interacting drugs can have affects on Metabolism- metabolised in the liver, numerous interactions with drugs that affect liver enzymes Absorption Protein binding- 99% protein bound and displacement increases plasma levels Pharmacodynamic Affect on bleeding risk without affecting INR e.g antiplatelet drugs, SSRI
Factors affecting INRPatient dependant factors • Heart failure INR increases in patients with exacerbations of HF due to dilution of clotting factors or hepatic congestion • Fever Increases INR (metabolic) in addition to abx/paracetamol interaction • Thyroid function Hyperthyroidism increases INR (metabolic) • Liver function Reduced production of clotting factors increases INR • Renal function Low albumin, uraemia. • Gastro-intestinal Disturbance Reduced intake Vit Kloss of clotting factors • Frail / elderly / Post op • Diet VariableVit K = unstable INR. High Vit K content of enteral feeds. • Alcohol “Binge drinking” increases INR.
Why warfarin is tricky and requires a collaborative approach Numerous drug interactions – need for clinic to be informed Narrow therapeutic window – risk of under & over-treatment if poorly controlled Requires regular therapeutic monitoring – avoiding missed tests Patient dependant factors- health status and life-style choices affect response GP responsible for prescribing not directly involved in dose adjustment
Advantages of warfarin Good evidence base for benefit Specific antidote(s) to reverse effectsin cases of bleeding, for emergency surgery, over-anticoagulation Regular monitoring supports patient adherence Cost effective. Estimate £180 per annum including monitoring in most areas. Consensus statement from Cardiac & Stroke Networks Lancashire & Cumbria recommends warfarin first line-line (publication imminent)
Comparison of bleeding rates Annual rates for bleeding event (fatal or non-fatal requiring hospital admission) following acute myocardial infarction (MI), according to anti-thrombotic therapy [adapted from Sorensen et al]
Patients on antiplatelet therapy who develop an indication for warfarin The following groups should normally stop antiplatelet therapy when warfarin is started Patients receiving an anti-platelet agent as primary prophylaxis for CVD Patients with peripheral artery disease or previous ischaemic stroke Patients on aspirin or clopidogrel as secondary prophylaxis with stable ischaemic heart disease (often defined as >12 months following acute myocardial infarction) Patients on a single antiplatelet agent <12 months following an ACS, should continue aspirin therapy until 12 months post ACS, unless they are regarded as having a high bleeding risk Patients on aspirin and clopidogrel, following an ACS or stent replacement should be carefully assessed for bleeding risk and discussed with their cardiologist, with a view to introducing warfarin and minimizing the duration of triple therapy. When combined warfarin and single antiplatelet agent are indicated, consideration should be given to use of aspirin given the higher bleeding risk associated with clopidogrel
Patients on warfarin who develop an indication for antiplatelet therapy Patients on warfarin who develop an acute ischaemic cardiac event eg ACS and individual’s risk / benefit needs to be assessed • Review need warfarin if low risk AF or short course for VTE and > 90 days and consider discontinuing warfarin. • Patients with a definite need to continue warfarin should be carefully reviewed and the minimum period of combination therapy used e.g If stents inserted-triple therapy with clopidogrel & aspirin for 4 weeks, followed by aspirin and warfarin to 12 months.
Advice to patients Patient counselling
NPSA OAT Packhttp://www.npsa.nhs.uk/nrls/alerts-and-directives/alerts/anticoagulant/
Advice to patients Treatment and Monitoring
Why warfarin is being recommended What their condition is Why warfarin is beneficial for their indication Opinion of the benefits of anticoagulation has changed over recent years see CHA2DS2-VASc How warfarin works for their indication E.g Warfarin reduces the risk of stroke in AF AF increases the risk of stroke: turbulent blood flow and incomplete emptying leading to areas of blood pooling which can lead to the formation of small clots which can cause stroke. Warfarin slows down clotting and reduces stroke. Patient decision aid NPC heritage site http://www.npc.nhs.uk/therapeutics/cardio/atrial/resources/pda_af.pdf
How to take warfarin Same time each day Not affected by food Different strengths are colour coded- don’t confuse number of milligrams with number of tablets Important to take it every day Do not double up if dose missed/ try to compensate e.g if dose usually taken at 6pm its OK to take it up to bedtime but not the next morning. Make a note of missed doses.
How it is monitored Why blood tests are important- safety & efficacy "Ideally we want your blood result to be between 2 & 3 this level will benefit you but not increase your risk of bleeding unacceptably” What the INR result means “we are timing to see how long your blood is taking to clot” Patients (used to BP or blood glucose measurements often don’t understand why we increase the dose for a low result How often blood tests might be required Initially once or twice a week. Average is 3-4 weeks or 6-12 weeks in stable patients
Potential adverse effects What side effects may occur Most people take warfarin without ill effect Report suspected adverse effects anticoagulant clinic or to your doctor How to recognise bleeding and the importance of seeking urgent medical attention should it occur Bleeding can be a sign that something has affected your warfarin treatment your blood is “too thin” or that you have an underlying cause of the bleeding which is worse because you take anticoagulants
How to achieve good anticoagulant control Other medication Regular medication has a consistent effect on warfarin Take “yellow” book to all doctors appointments Report changes to medications to anticoagulant clinic Buy non-prescriptions medicines from a pharmacy and inform them that you take warfarin Herbal medicines should be checked with the anticoagulant clinic-many increase bleeding risk
How to achieve good anticoagulant control Diet Consistency important Green vegetables are not dangerous but should be eaten as part as mixed diet Important the patient informs their clinic if they: Stop eating because of illness Advised to alter their diet by a doctor/dietician Experience nausea/vomitng/diarrhoea Prescribed dietary supplements Avoid cranberry juice
How to achieve good anticoagulant control General health People who are fit and well need more warfarin than people who are ill. Conversely, if a patient becomes seriously unwell there is an increased risk of high INR Patients must inform their anticoagulant clinic if they become seriously unwell
How to achieve good anticoagulant control • Alcohol Max 2 units for a woman and 3 for a man in any one day. Excess alcohol increases INR & increases risk of bleeding Alcohol abuse / excess associated with • High INRs • Missed tests • Low INR when doses missed • Increased bleeding risk- gastritis, varicies
Other advice Pregnancy Importance of adequate contraception in women of child-bearing age
How to obtain repeat prescriptions General practioners & dispensing pharmacist will ask to see your “yellow book” “To ensure that correct strength is prescribed and dispensed. So that your GP is assured that your results are reasonable and that you haven’t been missing your tests” The anticoagulant clinic has a systematic DNA procedure & we inform GP surgeries if more than on consecutive test is missed. We discharge patients who have missed more than four tests in a row. Please check with GP surgery & ourselves if prescriptions have been issued after a missed test.
Other advice Pregnancy Importance of adequate contraception in women of child-bearing age
Resources National Patient Safety Agency (NPSA) Alert No 18 Actions that can make anticoagulant therapy safer1 http://www.npsa.nhs.uk/nrls/alerts-and-directives/alerts/anticoagulant/ Learning pack available via CPPE Anticoagulation: managing patients, prescribing and problems
References • Guidelines on oral anticoagulation 4th edition. British Journal of Haematology 2011 http://www.bcshguidelines.com/documents/warfarin_4th_ed.pdf
Contacts East Lancs Hospitals Anticoagulant Clinics BGH office Telephone: 01282 804343 Email adrienne.lancaster@elht.nhs.uk