Download

1 / 14
170 likes | 489 Views
Intraoperative ECG Lead Placement. Brian Matthews SRNA Nicholas Stoddard SRNA David Perkins SRNA. Monitoring Basics. Impulse toward positive is an up swing; away from positive is down. J point, or “junction point”, is located at junction of S wave and start of ST segment.

E N D
Intraoperative ECG Lead Placement Brian Matthews SRNA Nicholas Stoddard SRNA David Perkins SRNA
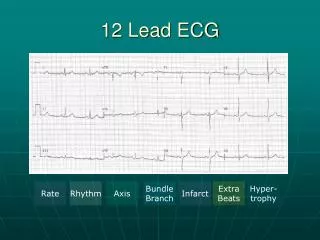
Monitoring Basics • Impulse toward positive is an up swing; away from positive is down. • J point, or “junction point”, is located at junction of S wave and start of ST segment. • ST segment is Measured 60 milliseconds from the J point. • 1mm change from baseline suggests myocardial injury.
Leads Bipolar and Augmented Placement(Frontal plane) • Bipolar leads read from negative to positive. • Bipolar leads are Lead I, II, and III also referred to as the limb leads. • Augmented leads read from center to specific + lead and are unipolar. • Augmented leads are aVR, aVL, and aVF.
Precordial Lead placement (Horizontal plane) • Unipolar leads, reading from center to outward. • V1: right sternal boarder 4th intercostal space V2: left sternal border 4th intercostal space V3: halfway between V2 and V4 V4: left 5th intercostal space, mid-clavicular line V5: horizontal to V4, anterior axillary line V6: horizontal to V5, mid-axillary line
Incidence/Indications • “The pooled results from the studies evaluating patients who had or were at risk of cardiac disease suggest that 3.9% (95% CI 3.3%–4.6%) of these patients experience major perioperative cardiac events.”
London et al 1988 • n-105 with CAD • Single lead monitoring unacceptable low • Leads II and V5 had 80% sensitivity • Leads II, V4, and V5 had a sensitivity of 96% for detecting ischemic events
Landesberg et al 2002 • n-185 major vascular surgery • Continual 12 lead monitoring during surgery • “We conclude that as a single lead, V4 discloses ischemia earlier, more frequently, and with a greater relative ST depression than the conventional V5” • Two lead monitoring is required to approach 95% sensitivity.
Martinez et al 2003 • n-149 Post-op ICU • “The majority of ischemia occurred in leads V2, V3, and V4, suggesting that the routine practice of monitoring leads II and V5 may not be optimal.”
Martinez et al 2003 • “Given that in routine ICU care leads II and V5 are usually monitored, we estimated that if all ischemic episodes occurring in either or both of these leads were detected, the maximal possible sensitivity of standard monitoring is 41% for detecting the first episode of ECG evidence suggestive of prolonged Ischemia”
12-lead “Fingerprinting” “First and foremost, if a preoperative 12-lead ECG has been done, “fingerprinting” of the tracing should serve as the primary guide for lead selection during the perioperaive period. If the baseline 12-lead shows significant primary ST-segment changes in leads V3,V4 and V5, then this lead set should be prioritized for continuous display in the operating room.” (Nagelhout, & Plaus, 2010) “A preoperative resting 12-lead ECG is recommended for patients with at least one clinical risk factor who are undergoing vascular surgical procedures and for patients with known CAD, peripheral arterial disease, or cerebrovascular disease who are undergoing intermediate-risk surgical procedures. A perioperative ECG is reasonable in persons with no clinical risk factors who are about to undergo vascular surgical procedures and may be reasonable in patients with at least one clinical risk factor who are undergoing intermediate-risk operative procedures” (Barash, et al. 2009)
Recommendations • If no pre-op 12 lead: then monitor Leads II and V3/V4. • With pre-op 12 lead available and normal; then the electrocardiographic lead with the most isoelectric ST level out of leads V3, V4, and V5 on the preoperative electrocardiogram is recommended or monitoring of ischemia. • If 12 lead available with ST changes, “fingerprinting”, monitor those specific leads.
Works Cited • Barash, P, Bruce, C, Robert, S, Cahalan, M, & Stock, M. (2009). Clinical anesthesia. Philidelphia: Lippincott Williams & Wilkins. • Devereaux, P, Goldman, L, Yusurf, S, Gilbert, K, & Leslie, K. et al (2005). Surveillance and prevention of major perioperative ischemic cardiac events in patients undergoing noncardiac surgery: a review. JMAC, 173(7), 779-788. • Landesberg, G, Mosseri, M, Wolf, Y, Vesselov, Y, & Weissman, C. (2002). Perioperative myocardial ishecmia and infarction. Anesthesiology, 96, 264-270. • London, M, Hollenberg, M, Wong, M, Levenson, L, & Tubau, J. et.al.(1988). Intraoperative myocardial ishemia: localization by continuous 12-lead electrocardiography. Anesthesiology, 69, 232-241. • Martinez, E, Kim, L, Faraday, N, Rosenfeld, B, & Bass, E. (2003). Sensitivity of routine intensive care unit surveillance for detecting myocardial ischemia. Critical care medicine, 31(9), 2302-2308. • Nagelhout, J, & Plaus, K. (2009). Nurse anesthesia. St. Louis, Missouri: W B Saunders Co.