Download
1 / 39
390 likes | 458 Views
Nutritional Supplementation and Serum Albumin Levels: Their Usefulness in Predicting and Improving Operative Morbidity and Mortality in the Geriatric Population. Amelia Crawford, PA-s2 October 28,2011. Preoperative Testing.

E N D
Nutritional Supplementation and Serum Albumin Levels: Their Usefulness in Predicting and Improving Operative Morbidity and Mortality in the Geriatric Population Amelia Crawford, PA-s2 October 28,2011
Preoperative Testing • Purpose is to identify underlying abnormalities or assess the severity of a current condition that may affect patient morbidity and mortality • For the geriatric patient, the clinician must strike a balance between routine testing and extensive evaluation.
Preoperative Testing • Best tools are history and physical exam: • Patient’s overall health • Cognitive Functioning • Nutritional Status • Family & Social Support • Medication Review
Routine Tests • CBC: • Hemoglobin- minimum of 9-10 mg/dl. • WBC- identify any infections or underlying myeloproliferative disorders • Basic Metabolic Panel: • Electrolytes: may be abnormal due to use of diuretics or ACEI/ARB • Creatinine Clearance- important for postop med dosing • Preop Serum Creatinine of >2.0mg/dl is a predictor of post op cardiac complications in patients undergoing non-cardiac surgery • Albumin level- assess nutritional status • Coagulation Studies: • PT, PTT, INR
Routine Tests • EKG: • For males>40-45 YOA & females>55 YOA, patients with systemic diseases like HTN, DM, PVD, hyperlipidemia, cerebrovascular disease, those taking medications that increase risk for cardiac toxicity • Helps identify patients with previous infarcts, which increases risk of complications • Chest X-Ray: • Patients >50 YOA & those cardiopulmonary or with pre-existing pulmonary disease • Risk of complications from anesthesia
Nutritional Assessment • Geriatric population is at risk for deficiencies because appetite and calorie consumption often decrease • In those with nutritional deficiencies there is sometimes concomitant depression, isolation, poor dentition, or excessive alcohol consumption • BMI: <18.5 is cause for concern • Healing is delayed in the presence of even mild protein calorie malnutrition. • Studies suggest that early recognition of protein malnutrition and initiation of nutritional therapy can shorten the length of hospital stays and improve patient outcomes • Serum albumin & pre-albumin are often used as nutritional status markers
Albumin Complex, high molecular weight protein produced by the liver Widely used in nutritional assessment Half-life of 18-20 days • Normal value: 3.30 to 4.80 g/dL • Affected by many factors including dehydration, inflammation, hepatic and renal dysfunction • The level typically takes 14 days to return to normal when the pool has been depleted.
Pre-albumin • A serum and cerebrospinal fluid carrier of the thyroid hormone thyroxine (T4) and retinol, produced mainly by the liver. • Lower levels correlates with protein malnutrition (within 1 week of change in nutrient intake). • Not affected by dehydration but systemic inflammation does cause a decrease. • Clinical studies indicate that determination of the pre-albumin level may allow for earlier recognition of and intervention for malnutrition. • Synthesis of pre-albumin increases above baseline levels within 48 hours of protein supplementation in patients with protein calorie malnutrition and returns to normal levels within eight days. • ½ life of 2-3 days • Normal level: 16-35 mg/dL
Preoperative Serum Albumin Level as a Predictor of Operative Mortality and Morbidity Gibbs et al. Archsurg. 1999; 134; 36-42
Background Information • Hypoalbuminemia has been shown to be associated with increased mortality and morbidity rates in hospitalized and community dwelling elderly persons. • Hypoalbuminemia has also been associated with adverse outcomes after surgery.
Objective • To improve precision and reliability of estimates of the association between preoperative serum albumin concentration and surgical outcomes
Design • Prospective observational study • Setting: 45 VA medical centers • Patients: 54,215 major non-cardiac surgery cases from the National VA Surgical Risk Study • 97.1% male • Mean age was 61 years • 76% white, 18% black, 6% other ethnicities • General surgery (28.3%), Orthopedic (18.0%), Urology (14.8%), Vascular (11.7%), Neurosurgery (8.4%), Thoracic (7.3%), ENT (5.9%), Plastic (3.7%), Other (2.0%) • Data collected until 30 days post-operatively
Design • Independent Variables: • 1. Serum albumin values closest to the day of the surgery (within 30 days) • Dependent Variables: • 1. Operative Mortality: death due to any cause within 30 days of the operation • 2. Operative Morbidity: 21 of the predefined complications recorded within 30 days of the operation.
Primary Outcome • 30 day operative mortality and morbidity
Stastical Analysis • Univariate Analyses- association between preoperative serum albumin levels and mortality and morbidity. Compared the predictive ability of albumin level with that of each of 61 other preoperative variables. • Multivariant Logistic Regression Analyses- assess the predictive ability of albumin level independent of the effects of other variables. • Complication-Specific Analyses- association between preoperative serum albumin and each of 21 pre-defined complications
Results • Univariate Analysis: • 1. Albumin level was the best predictor of 30 day mortality and morbidity. • 2. Albumin level alone correctly discriminated between survivors and non-survivors 78% of the time • For all operations, the mortality rate increases from less than 1% for albumin levels of 46g/L or higher to 28% for albumin levels below 21g/L
Results • Multivariate Analyses: • Albumin level is the strongest predictor in both mortality and morbidity models for all operations and in several subspecialty models • Odds ratios for albumin level in all operations models indicate that a decrease of 10g/L in albumin value was associated with more than a 2 fold increase in the odds of dying and almost a 2 fold increase in the odds of a complication.
Results • Complication-Specific Analysis: • Albumin level was a relatively strong predictor of most of the complications: • particularly systemic sepsis, failure to wean off the ventilator, and pneumonia
Results • Separate analyses were performed for a lower risk segment of the sample and for women, and there was a negative association between serum albumin level and 30 day mortality for both groups.
Summary of Results • A decrease in serum albumin from concentrations greater than 46g/L to less than 21g/L was associated with an increase in mortality rates from less than 1% to 29% and in morbidity rates from 10% to 65%. • In regression models, albumin level was the strongest predictor of mortality and morbidity as a whole and within several subspecialties (independent of the effects of other risk variables) • Albumin level was a better predictor of some types of morbidity, particularly sepsis and major infections.
Perioperative Oral Nutritional Supplements in Normally or Mildly Undernourished Geriatric Patients Submitted to Surgery for Hip Fracture: A Randomized Clinical Trial Carretero et al. Clinical Nutrition October 2010 Vol. 25; issue 5: 574-579
Objectives • To study whether perioperative administration of oral nutritional supplements (ONS) are effective in geriatric patients undergoing surgery for hip fracture, starting at admission.
Design • Randomized control trial • Patients: • 60 patients total • >65 YOA • Admitted between May 2005 and September 2008 due to hip fracture and underwent hip surgery • No patients had been on ONS or received any other nutritional support within the previous 6 months • All patients had similar baseline characteristics
Exclusion Criteria • 1. Moderate to severe malnutrition: • Weight loss of > 5% in the previous month or >10% in the previous 6 months of their usual body weight • ARF, CRF, Hepatic Insufficiency or Cirrhosis, Stage III or IV HF, Repiratory Failure, GI conditions that precluded the use of ONS
Interventions • Control Group (n=30): no intervention • Intervention Group (n= 30): Perioperative ONS initiated at admission and maintained until discharge • 2 Fortimel 200mL bricks which provided 20g protein & 200 kcal • Amount of ONS and diet consumed by the patient was measured after every meal. • Blood testing and body measurements were done at baseline, 48 hrs after surgery, then weekly, and also at hospital discharge. • Normal ranges: • Serum albumin = 3.3-5.2g/L • Pre-albumin = 20-40mg/dL • RBG are as follows= 3.0-6.0mg/dL
Outcomes • Primary: • 1. Change in albumin, pre-albumin, and retinol binding globulin. • 2. Changes in weight, BMI, mid-brachial circumference, and tricipital fold • Secondary: • 1. Length of hospital stay • 2. Postoperative complications
Statistics • Comparisons between both groups at baseline were performed using the independent Student t test, Mann-Whitney U test, or Chi-Square test • General linear model was used for the comparison of continuous variables throughout the study • Backwards multiple logistic regression model was employed to study the effects of multiple independent variables on the occurrence of post-operative complications
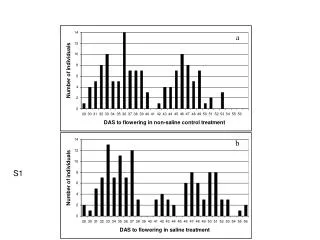
Results • Primary Outcomes: • There was a significant change in albumin between the 2 groups (F=22.536, P<0.001) from the time of admission until the time of discharge, with the control group demonstrating a larger decrease in serum albumin and worse post-op recovery compared to the ONS group. • Serum pre albumin also demonstrated similar significant changes (F=6.654, P=0.001) • RBG demonstrated a similar change, but this difference was not significant (F= 2.281, p=0.089) • No significant differences in the change in BMI (F=2.509, P=0.089), tricipital fold (F=0.584, P=o.636), or the mid-brachial circumference(F=0.031, P=0.864) between the groups.
Results Open circles = control group Filled circles= ONS group
Results • Secondary Outcomes: • Length of postoperative hospital stay was similar in the 2 groups (p= 0.664) • No significant difference in postoperative complication rates between the 2 groups (p= 0.091) • Non-significant tendency for higher postoperative complication rate in the control group, but no specific complication could be identified as predominant in either group.
Results • Ancillary Analyses: • Backwards multiple logistic regression analysis with the occurrence of postoperative complication as the dependent variable and age, gender, baseline BMI, mid-brachial circumference & tricipital fold, non-protein, and supplemented proteins per day as covariates. • The supplemented proteins per day was determined to be a predictive variable ( OR= 0.925; 95% CI; P= 0.003) • Suggests that higher protein intake is associated with a smaller risk of postoperative complications
Conclusions • Perioperative administration of ONS is effective in increasing serum proteins in nourished or mildly nourished geriatric patients who undergo surgery for hip fracture. • Patients with higher protein intakes had fewer postoperative complications
Final Comments • Serum albumin and pre-albumin levels are used frequently to monitor nutritional status. • However, these markers are affected by more than just protein nutrition. • Levels should be interpreted along with weight, BMI, physical exam, and other labs. • They are cost effective labs that can help predict the risk of postoperative morbidity and mortality in geriatric patients • In geriatric patients undergoing surgery, correcting nutritional deficits before and after surgery can help prevent complications and improves mortality rates.
References • Shenkin, Alan. Serum Prealbumin: Is It a Marker of Nutritional Status or of Risk of Malnutrition? Clin. Chem., Dec 2006; 52: 2177 - 2179. • Beck FK, Rosenthal TC. Prealbumin: a marker for nutritional evaluation. Am Fam Physician. Apr 2002; 15;65(8):1575-8. • Woogler, JM. “Preoperative Testing and Medication Management.” Clinics in Geriatric Management, Nov 2008; 24 (4): 573-583. • Carretero et al. Perioperative oral nutritional supplements in normally or mildly undernourished geriatric patients submitted to surgery for hip fracture: A randomized clinical trial. Clinical Nutrition, Oct 2o1o; 29 (5):574-579 • Gibbs et al. Preoperative Serum Albumin Level as a Predictor of Operative Mortality and Morbidity. Arch Surg. 1999;134:36-42