Download
1 / 46
460 likes | 609 Views
Disorders of Neural Tube Closure. Jan M. Eckermann, MD, PGY-3 Department of Neurosurgery Loma Linda University Medical Center. Review of Neuroembryology. Dorsal induction Primary neurolation: 3-4 wks gestation Brain and upper spine

E N D
Disorders of Neural Tube Closure Jan M. Eckermann, MD, PGY-3 Department of Neurosurgery Loma Linda University Medical Center
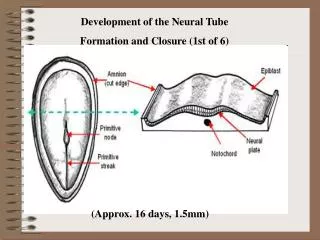
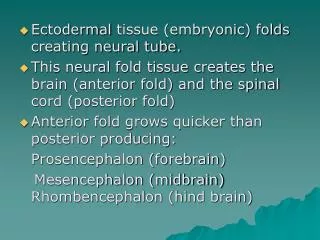
Review of Neuroembryology • Dorsal induction • Primary neurolation: 3-4 wks gestation Brain and upper spine • Secondary neurolation: 4-5 wks gestation Distal spine
Disorders of neural tube closure • Chiari I-IV • Encephaloceles • Anencephaly • Corpus Callosum Agenesis • Spinal Dysraphism (Spina bifida) • - Menigoceles • - Myelomeningoceles • Tethered chord
Chiari I ANATOMY • Peglike cerebellar tonsils displaced into upper cervical canal ( >10mm) • HCP 25% • Syringomyelia 60% • Skeletal anomalies 25%
Chiari I Clinical • Asympotmatic (30%) • Headache • Weakness • Cerebellar signs • Herniation >12mm invariably symptomatic
Chiari I Treatment • Observation if asymptomatic • Surgery if symptomatic: p-fossa decompression +- cervical laminectomy
Chiari II Anatomy • Calvarial defects “Lueckenschaedel” • Small p-fossa • Fenestrated falx • HCP in 90% • Myelomeningocele in 100% • Syringohydromyelia in 50%-90%
Chiari II Clinical • Dysphagia • Apneic spells • Stridor • Aspiration • Arm weakness
Chiari II Treatment • Shunt • P-fossa decompression • Repair of MM
Chiari III and IV Chiari III Most severe form. Chiari II + low occiptial or high cervical encephalocele. Usually incompatible with life Chiar IV Severe cerebellar hypoplasia or absence. No herniation Extremely rare
Enephaloceles • Anatomy • Failure of the anterior neural tube to close due to genetic, infection, or toxic reasons. • 1/1000 • Distorted parts of the (covered) brain protruding extracalvarially
Encephalocele Anatomy Occipital 90% Parietal 10% Transsphenoidal Frontoethmoidal Nasal
Encephaloceles • Parietal encephalocele • Frontoethmoidal encephalocele
Encephaloceles • Clinical Depends on involvement • Treatment Surgical excision of sac with water-tight dural closure
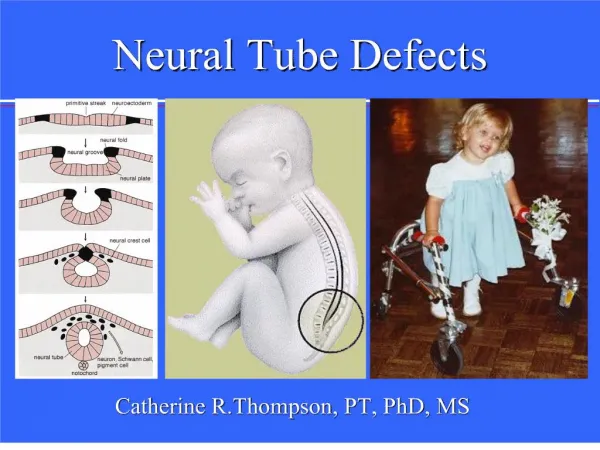
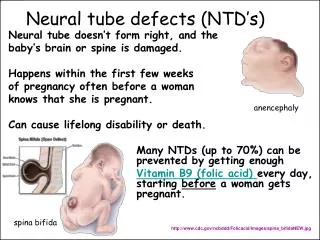
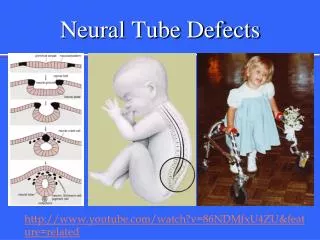
Anencephaly • 1/1000 • Anencephaly is a defect in the closure of the neural tube during fetal development. • Large defect of the calvarium, meninges, and scalp. • Incompatible with life.
Corpus Callosum Agenesis • Expansion of third ventricle • May present with HCP, seizures • May be incidental finding without any clinical significance
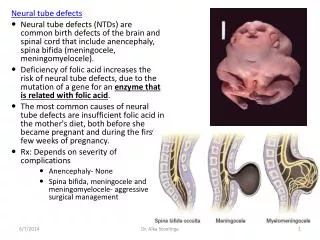
Spinal Dysraphism (spina bifida) • Spina bifida occulta: 20-30% in North Americans, often incidental, cutaneous manifestations • Spina bifida aperta: • Meningocele • Myelomeningocele
Spinal Dysraphism • Spina bifida occulta
Spinal Dysraphism • Meningocele
Spinal Dysraphism • Myelomeningocele
Meningocele • 1-2/1000 • 1/3 have neurological deficits • Surgical repair with water-tight dural closure
Meningomyelocele • 1-2/1000 live birth • Failure of complete closure of caudal neural tube • 85% occur in lumbar region
Myelomeningocele • Clinical • Mild to complete LE paralysis • Ruptured vs unruptured • Urinary incontinence • Skeletal abnormalities
Myelomeningocele • Treatment • If open, Gent and Naf IV • Prone, bottom up • Telfa with wet gauze over lesion • Surgical closure within 36hrs • Shunt if overt HCP • Urologic and Orthopaedic consultation
Lipomyelomeningocele • Present with back mass, bladder problems, paralysis • Cutaneous stigmata • Symptoms are due to tethered cord and cord compression from fatty mass • Treatment is surgical decompression
Tethered Cord Syndrome • Anatomy • Low conus medullaris • Short, thick filum terminale • Intradural lipoma
Tethered Cord Syndrome • Clinical • Cutaneous findings • Gait difficulties • Visible muscle atrophy • LE sensory deficits • Bladder dysfunction • Scoliosis
Tethered Cord Syndrome • Treatment • Laminectomy with division of filum terminale • Removal of lipoma if present • Followed with MRI