Comprehensive Tuberculosis Treatment Card for Patient Beti Magdalene: Documentation and Management
This document outlines the treatment plan for Beti Magdalene, a patient diagnosed with pulmonary tuberculosis. It includes patient demographics, treatment history, prescribed medications, and monitoring instructions. The treatment follows the Botswana National Tuberculosis Programme guidelines, detailing drug combinations, dosing, and patient category. Important notes are provided regarding drug side effects and dosage adjustments. Regular sputum examinations and chest X-rays are scheduled for effective monitoring of treatment outcomes. Adherence to the drug administration schedule is crucial for recovery.

Comprehensive Tuberculosis Treatment Card for Patient Beti Magdalene: Documentation and Management
E N D
Presentation Transcript
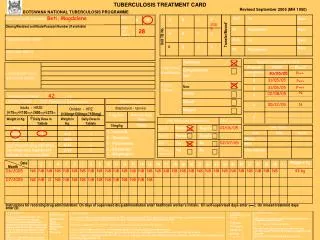
TUBERCULOSIS TREATMENT CARD Name (surname, first name) Beti, Magdalene Sex OUT To Date M F A B C D 2005 Omang/Resident certificate/Passport Number (if available) Age (in years) IN Registered Date Physical Address (in full) A B C D Unit TB No. OUT To Date B C D Date IN Registered Alternative address TuberculosisClassification Pulmonary Pre-treatment history and clinical findings Patient Category3 Pre-treatment Weight_____42_______Kg Failure I. INITIAL PHASE – (FDC- Fixed Dose Combinations) Reserve Drug Default Adults - HRZE(H75mg+R150mg+Z400mg+E275mg) Children - HRZ(H30mg+R60mg+Z150mg) Streptomycin - 1gm vial Daily Dose Maximum Daily Dose Relapse Weight in Kg. Daily Dose in Tablets Weight in Kg. Daily Dose in Tablets 750mg 15mg/kg 30-39 2 ≤7 1 H – Isoniazid R – Rifampicin Z – Pyrazinamide E – EthambutolS – Streptomycin 40-54 3 8-14 2 ≥55 4 15-19 3 Note: If severe drug side-effect, use single dose regimen and indicate in the remarks field 20-24 4 25-29 5 Revised September 2005 (MH 1050) BOTSWANA NATIONAL TUBERCULOSIS PROGRAMME 28 Transfer/Moved1 A Sputum Examination for AFB At month Date of Collection Result4 Extrapulmonary Site2:_____________________ 30/05/05 P+++ (pretreatment) 0 31/05/05 0 P+++ New 31/05/05 P+++ 0 N 02/08/05 2 6 05/12/05 N 8 Date Month Instructions for recording drug administration: On days of supervised drug administration enter healthcare worker’s initials; On self-supervised days enter (▬); On missed treatment days enter (0)
No. Expected No. Screened 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Weight in Kg CONTINUATION PHASE CONTACT SCREENING CULTURE & SENSITIVITY REPORTS TREATMENT OUTCOMES CHEST X-RAY Date Month Instructions for recording drug administration: On days of supervised drug administration enter healthcare worker’s initials; On self-supervised days enter (▬); On missed treatment days enter (0)