Case scenario
An analysis of early insulin glargine added to metformin with or without sulfonylurea: impact on glycaemic control and hypoglycaemia. Case scenario.


Case scenario
E N D
Presentation Transcript
An analysis of early insulin glargine added to metforminwith or without sulfonylurea: impact on glycaemic controland hypoglycaemia
Case scenario • The patient is 45 years old man , is known case of type 2 diabetes from 3years ago with inadequate glycaemic control , who treated with metformin , and admitted here for control of diabetes
PICO • P : Patient with type 2 diabetes with inadequate glycaemic control • I : early insulin glargine adding • C : later insulin glargine adding • O : glycaemic control and hypoglycaemia
Keywords • Type 2 DM • Early insulin therapy • Basal insulin
Introduction • In 2009 • American Diabetes Association (ADA) • European Association for the Study of Diabetes (EASD) • Consensus statement on the initiation and adjustment of therapy for type 2 diabetes
Introduction • Glycaemic control HbA1c <7.0% • These tier 1 interventions included lifestyle modification and metformin (MET) concomitantly initiated at step 1
Introduction • The addition of either basal insulin or sulfonylurea (SU) therapy to MET at step 2 (if glycaemic goals are not achieved with MET alone)
Introduction • the addition or intensification of insulin therapy as needed to attain glycaemic control at step 3
Introduction • In routine clinical practice • Insulin therapy is more often initiated after two or more oral antidiabeticdrugs (OADs) have proven inadequate to achieve or maintain glycaemiccontrol.
Introduction • The reasons for delaying insulin initiation are varied, but may include • patient and physician perceptions • Insulin therapy regimens are too complex self administering injections • Fears regarding side effects such as hypoglycaemiaand weight gain.
Introduction • For these reasons, we sought to use the extensive clinical trial database of insulin glargine to assess the observed clinical outcomes of earlier versus later basal insulin initiation on glycaemiccontrol and safety after 24 weeks of treatment.
Introduction • to compare clinical outcomes after initiating insulin glargine in patients with uncontrolled type 2 diabetes on 0 or 1 OAD versus 2 OADs at baseline • We also performed a meta-analysis to evaluate the robustness of the pooled analysis and to control for differences in sample size.
Methods • In total, 63 randomized controlled trials evaluating insulin glargine in patients with type 2 diabetes • These studies were performed between 1997 and 2007 • Individual patient data were available for inclusion in pooled analyses.
Methods • prospective, randomized, controlled trials of ≥24 weeks’ duration • Enrolled adult patients with type 2 diabetes with inadequate glycaemic control • Basal insulin was given once daily, with no concomitant prandial or bolus insulin administration
Methods • Insulin glargine was initiated at 10 U/days and dose adjustment to achieve fasting plasma glucose levels <100 mg/dl • Studies were conducted according to Good Clinical Practice and in accordance with the Declaration of Helsinki.
Methods • Twelve studies met these eligibility criteria; however, one study discontinued thiazolidinediones abruptly at baseline and was not included in this analysis. • Therefore, data from 11 studies were used in the pooled analysis
Clinical Outcomes • Week 24 HbA1c level and change from baseline • The percentage of patients reaching a target HbA1c level of ≤7.0%, • Change in body weight from baseline • Insulin dose at endpoint • Symptomatic and severe hypoglycaemic incidence
Clinical Characteristics and Patient emographics • Of 3801 patients, a total of 2171 in the 11 selected studies were treated with insulin glargine and therefore inclusion in the pooled analysis. • 1.8% of patients were taking no OAD • 45.2% took 1 OAD • 52.2% took 2 OADs • 49.9% of all patients were taking MET + SU • 36.5% of patients took an SU only • 8.5% took a MET only.
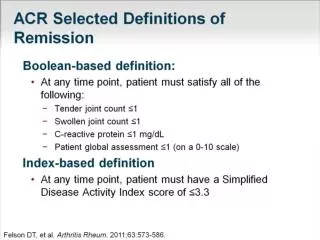
Glycaemic Outcomes • HbA1c ≤ 7.0% at week 24 after the addition of basal insulin • Results were similar between the 0/1 OAD group and the 2 OAD group (54.7% vs. 56.7%, respectively, p = 0.0541). • MET-only group (68.1%) other groups (50.4 and 56.4% for SU only and combination groups). • MET-only group experienced the largest mean improvement in HbA1c from baseline
Weight Change • Weight gain from baseline to week 24 was not significantly different • The MET-only group had the numerically lowest weight gain over 24 weeks after basal insulin initiation.
Insulin Dose • The stable weight-based insulin doses for patients on 0/1 OAD and on 2 OADs were similar • The mean insulin dose per kilogram in patients on MET only was higher than that for patients on SU only or on SU + MET combination therapy
Hypoglycaemia • Symptomatic • Confirmed symptomatic: glucose <50 mg/dl • Severe hypoglycaemia • Incidence and rates were low overall
Discussion • Patients taking MET alone • The greatest HbA1creductions. • largest proportion of patients achieving glycaemic goal. • The lowest rate of symptomatic and severe hypoglycaemia. • The lowest weight gain.
limitation • only studies of insulin glargine • outcomes following 24weeks of treatment • We did not assess if any changes did occur in OADs during the course of this study
Materials and Methods The Medline, Embase and Cochrane Library electronic databases were searched English language papers from January 2000 to August 2010
Inclution criteria: primary studies in adults with T2DM with insulin being at least one of the interventions (ii) studies concerned with insulin initiation and intensification, (iii)Randomized clinical trials, observational studies, economic evaluations, systematic reviews and meta-analyses, (iv)At least one baseline and post-treatment efficacy, quality of life (QoL), safety and economic outcomes of interest
outcome (i) change from baseline in HbA1c (ii) change from baseline in BG (iii) QoL/treatment satisfaction (TS) (iv) rate of hypoglycaemia, (v) change from baseline in weight (vi) economic cost
Study Characteristics 40 studies were included 27 were randomized controlled trials (RCTs), 11 were observational studies 2 were modelling studies.
Patient Characteristics Most of the studies included patients with ages ranging from 30 to 80 years. In a majority of studies, the mean HbA1c level at baseline was >7% with values ranging from 7.5 to 12%. The body mass index (BMI) of included patients was ≤35 kg/m2, except for a few studies that included patients with BMI ≤ 40 kg/m2.
Clinical Outcomes HbA1c at baseline and endpoint were reported in 37 of the 40 included studies The mean reduction in HbA1c levels was more than 1% in all patients initiating insulin therapy The mean HbA1c reduction was significantly more in patients on insulin or insulin added to OADs compared to patients on OADs alone Early initiation of insulin therapy was associated with greater reductions in HbA1c levels from baseline.
Quality of Life were reported in six studies and was the primary outcome of one study. No significant difference was reported for QoL outcomes between insulin and OADs similar for OADs alone vs. OADs in combination with insulin
Adverse events Hypoglycaemia and weight gain were the main adverse events that were reported in most studies Hypoglycaemic rates or events were reported to be lower with insulin initiation as compared to OADs alone Incidence of hypoglycaemic events was similar for the insulin types
Adverse events Weight gain was observed with all insulin across studies There were different reports regarding weight gain for studies comparing OADs alone and insulin initiation -3.36 kg gained with insulin + metformin - 10.10 kg gained with triple OADs Similar weight gain for OADs and insulin No weight gain with OADs compared with insulin initiation