Acute Pancreatitis: Diagnosis, Management & Complications
Understand acute pancreatitis: causes, assessment of severity, investigations, treatment, and complications.

Acute Pancreatitis: Diagnosis, Management & Complications
E N D
Presentation Transcript
CASE SCENARIO History A 50-year-old civil services officer presents to the A&E with 2-days h/o vomiting and epigastric pain which radiates through to the back. He is not on any regular medication, but admits to drinking alcohol everyday for the last five years.
CASE SCENARIO Examination The patient is unable to lie flat for the examination. His blood pressure is 150/80 mmHg and he has a pulse rate of 120/min. Palpation of his abdomen reveals tenderness in theepigastrium. The abdomen is not distended and he has normal bowel sounds. Rectal examination is unremarkable.
CASE SCENARIO Investigations
QUESTIONS • What is the most likely diagnosis? • Which important differential diagnosis should be excluded? • How will you grade the severity of the condition? • What are its causes? • What are the other causes of the elevated serum marker of this condition? • How will you manage the condition?
ACUTE PANCREATITIS Faisal Ghani Siddiqui MBBS; FCPS (General Surgery); PGDIP-BIOETHICS; MCPS-HPE; FICLS; (MHPE)
PANCREATITIS -inflammation of the gland parenchyma of the pancreas
WHAT IS ACUTE PANCREATITIS? • Acute inflammation of pancreatic parenchyma • Presents as an emergency • With abdominal pain and vomiting • Associated raised pancreatic enzyme levels in blood or urine
ACUTE PANCREATITIS –CLINICAL FEATURES • Pain • Vomiting • Tachypnea, tachycardia, shock • Fever • Jaundice • Abdominal distension • Grey Turner / Cullen’s sign
Cullen’s sign Grey-Turner’s sign
ACUTE PANCREATITIS –INVESTIGATIONS • Laboratory investigations • Serum amylase / lipase levels • Radiological • Plain X ray abdomen (Ileus; calcifications) • X-ray chest (pneumoperitoneum; pleural effusion)) • Ultrasound (gallstones; pancreatic edema) • Contrast enhanced CT (Pancreatic necrosis)
OTHER CAUSES OF HYPERAMYLASEMIA • Perforated peptic ulcer • Mesenteric infarction • Acute cholecystitis • Generalized peritonitis • Intestinal obstruction • Ruptured ectopic pregnancy • Diabetic ketoacidosis • Bowel perforation • Renal failure • Ruptured aortic aneurysm
Colon cut-off sign
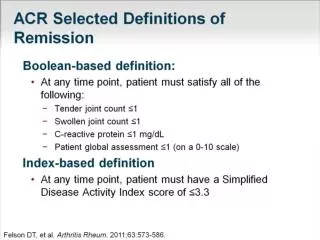
ASSESSMENT OF SEVERITY –SCORING SYSTEMS • Ranson’scriteriae • Used to grade severity • Helps decide whether patients should be managed • on ward, or • in HDU or intensive care
RANSON’SCRITERIAE On admission: • Age: >55 years • WBC count: >16 x 109 L • LDH: >600 IU/L • AST: >120 IU/L • Glucose: >10 mmol/L • Fluid sequestration: >6 L Estimates on mortality are based on the number of points scored: 0–2: =2 per cent; 3–4: =15 per cent; 5–6: =40 per cent; >7: =100 per cent Within 48h: • Hematocrit fall: >10 per cent • Urea rise: >0.9 mmol/L • Calcium: >2mmol/L • pO2: >60 mmHg • Base deficit: >4
ASSESSMENT OF SEVERITY –OTHER SCORING SYSTEMS • Glasgow • APACHE-II
ACUTE PANCREATITIS -MANAGEMENT • NPO • Analgesics • Fluid resuscitation • Supplement oxygen • Antibiotics • Continuous monitoring for systemic / local complications • Treat the cause
ACUTE PANCREATITIS- COMPLICATIONS Local • Sterile pancreatic necrosis • Infective pancreatic necrosis • Pancreatic abscess • Pancreatic pseudocyst • Abscess formation • Splenic / portal vein thrombosis Systemic • Renal failure • Respiratory failure • Cardiac failure • Septic shock • Multi-organ failure and death
CASE SCENARIO History A 50-year-old civil services officer presents to the A&E with 2-days h/o vomiting and epigastric pain which radiates through to the back. He is not on any regular medication, but admits to drinking alcohol everyday for the last five years.
CASE SCENARIO Examination The patient is unable to lie flat for the examination. His blood pressure is 150/80 mmHg and he has a pulse rate of 120/min. Palpation of his abdomen reveals tenderness in the epigastrium. The abdomen is not distended and he has normal bowel sounds. Rectal examination is unremarkable.
CASE SCENARIO Investigations
QUESTIONS • What is the most likely diagnosis? • Which important differential diagnosis should be excluded? • How will you grade the severity of the condition? • What are its causes? • What are the other causes of the elevated serum marker of this condition? • How will you manage the condition?