Download

1 / 56
740 likes | 2.18k Views
Development of the heart. Dr Rania Gabr. oBJECTIVES. Describe the formation and position of the heart tube. Explain the mechanism of formation of the cardiac loop. Discuss the development of sinus venosus . Explain how cardiac septa are formed.

E N D
Development of the heart Dr Rania Gabr
oBJECTIVES • Describe the formation and position of the heart tube. • Explain the mechanism of formation of the cardiac loop. • Discuss the development of sinus venosus. • Explain how cardiac septa are formed. • Describe the septum formation in the common atrium. • Discuss the septum formation in the Atrioventricular canal. • Discuss the septum formation in the Truncusarteriosus and BulbusCordis • Describe the septum formation in the ventricles.
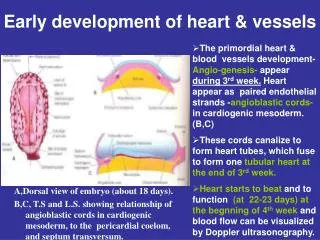
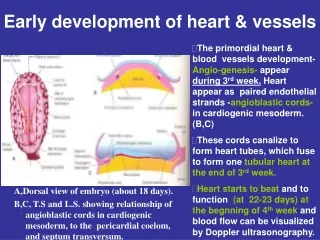
Angiogenesis • The vascular system as well as the blood elements are Mesodermal in origin. • The splanchnic mesodermal cells proliferate and form cell clusters called “angiogenic clusters” or “blood islands” which lie in front and on either side of the anterior part of the embryonic disc.
Formation of the Cardiogenic field Clusters of angiogenetic cells form a "horseshoe-shaped" cluster anterior and lateral to the brain plate.
Origin of the heart tube: Mesoderm of the cardiogenic plate at the 3rd week.
Development: • It starts by the formation of 2 heart tubes each has a cranial end and a caudal end. • - The cranial end is the arterialend and is connected to the aortic sac then to dorsal aorta, • and the caudal end which is the venous end (embedded in the septum transversum).
This venous end (caudal end) receives 3 veins for each tube; they are: 1- umbilical, 2- vitellineand 3- common cardinal veins. • - Fusion of the 2 heart tubes occurs. This fusion occurred in a cranio-caudal direction leads to the formation of single heart tube.
- The newly formed heart tube(1tube) has an arterial end (cranial end)connected to the dorsal aorta and • A caudal end (venous end) (embedded in the septum transversum) receives 3 pairs of veins, they are: • 1-umbilical • 2-vitelline and • 3-common cardinal veins
- The clusters form endothelial vessels which fuse to form the right and left endocardial heart tubes - As a result of folding of embryo in transverse direction the two endocardial heart tubes come close to each other and fuse to form single endocardial tube
Lateral folding Lateral folding results in fusion of the caudal portion of the paired endocardial tubes
Lateral body folding occurs as well as head folding. • - The heart tube bulges into the dorsal surface of the pericardial cavity • - It is suspended by dorsal& ventral mesocardiumwhich disappear Pericardial cavity Dorsal mesocardium
The heart tube continues to elongate forming the cardiac loop. • -The cardiac loop invaginates in the pericardial cavity. • -Hence the heart is covered by 2 layers of the pericardium: visceral layer internally and parietal one externally and in between lies the pericardial cavity. hhhhhhhhhhh llkj bbb
- The pericardial cavity hangs by the dorsal mesocardium. • - Degeneration of the dorsal mesocardium leads to formation of transverse sinus of pericardium which is a cavity between the arterial and venous ends of the heart tube.
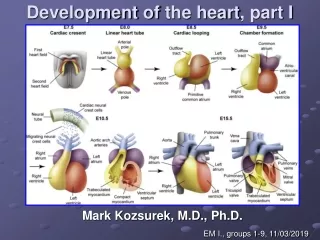
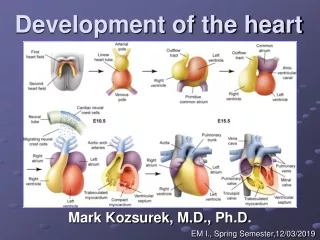
2 constrictions appear in this tube dividing the heart tube into 3 chambers externally, those chambers are: • Bulbuscordiscranially • Ventricle caudal to it, • Atrium caudal to the ventricle. • - The grooves from above downward are: • 1-Bulbo-ventricular groove. • 2-Ventriculo-atrial groove.
The bulbuscordis is elongated and form the truncusarteriosus. • - At the venous end another groove appears and separates the atrial part from the sinus venosus. This groove is called • 3-sino-atrial groove..
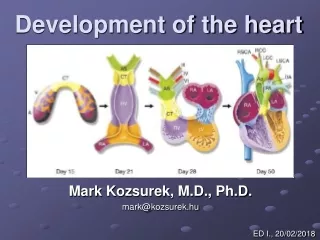
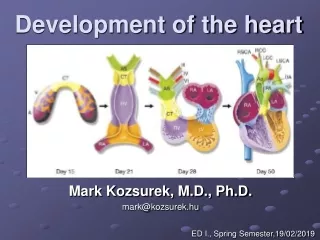
1st aortic arch Parts of the Heart Tube Chambers of the heart tube: • Three grooves are formed in the tube will form four chambers: • Sinus venosus, Primitive atrium, Primitive ventricle and Bulbuscordis.
---“S”-shaped heart: The heart tube continues to grow and bend, atrium shifts in the dorso-cranial direction; sinus venoususlocated at caudal portion of atrium.
Development of the sinus venosus • The sinus venosus receives venous blood from the right and the left horns. • Again each horn receives 3 veins: umbilical-vitelline and common cardinal veins. • The sinus is widely connected to the primitive atrium. through the Sino-atrial orifice. jjjjjj
Venous blood drainage shifts from left to the right side. • The communication between the sinus and the atrium is shifted to the right. • The right umbilical vein and the left vitelline vein are obliterated during 5thweek • Left common cardinal vein is obliterated at 10th week. • The left sinus horn regresses, and what remains only oblique vein of left atrium and coronary sinus. • Right sinus horn is enlarged and incorporated into the right atrium, to form the smooth-walled part of right atrium.
Septum Formation in Common Atrium End of Fourth Week Formation of septum primum- sickle shaped crest from the roof of common atrium Ostium primum- opening between the lower rim of septum primum and endocardial cushion
An extension is growing from the endocardial cushions, closing the ostiumprimum, but before that, a new opening appears in the upper portion of septum primum, that is ostiumsecundum. • Later, a new septum develops to the right of septum primum, • that is septum secundum, • which is a crescent shaped , incomplete partition, with an opening inferiorly, that is foramen ovale.
---before birth, blood can flow from the right atrium towards the left atrium • ---after birth, the two septa fuse to separate the atrium completely
Further Differentiation of the Atria Right Atrium- Embryonic R atrium - trabeculated atrial appendage Sinus venarum(smooth walled part) from R sinus horn Left Atrium Embryonic L atrium-trabeculated atrial appendage Smooth walled part from pulmonary vein
In 25% of normal population, the • foramen ovale remains ‘probe patent’.
Development of the right atrium: - It is formed of 2 parts: 1. Smooth part, which is formed from absorption of the right horn of sinus venosus to be a part of the right atrium. 2. Rough part, originated from the primitive atrial chamber of the heart tube. Development of the left atrium: - It is formed of 2 parts: 1.Smooth part, which is formed from absorption of the pulmonary vein to be a part of the left atrium. 2.Rough part, originated from the primitive atrial chamber of the heart tube.
After birth foramen ovale is closed by: • 1- A decrease in Rt. atrial pressure due to occlusion of placental circulation • 2- An increase in Lt. atrial pressure due to increased pulmonary venous return. • Septum primumis pushed andfuses with septum secundumto form interatrial septum • Lower margin of septum secundum forms annulus ovalis • - Septum primum forms floor of fossa ovalis
Septum in the atrio-ventricular canal • Superior and inferior endocardial cushions fuse , to form a partition dividing the canal into right and left atrioventricular canals. • Two lateral cushions appear on the right and left. • Each atrioventricularorifice is surrounded by local proliferations of mesenchymal tissue, these form the valves, under which the tissues are vacuolated, but the valves remain attached to the ventricular walls by cords of the papillary muscles.
Division of Atrioventricular canal day 30 embryo day 35 embryo
Septum in the truncusarteriosus and Bulbuscordis • During 5th week, two opposing ridges appear in the truncus, which are also called truncus swellings or cushions, one superior and to the right and the other is inferior and to the left. • These swellings grow distally in spiral way, or twisting around each other. • Fusion of the truncus swellings results in formation of aorticopulmonary septum, which divides the truncus into aortic and pulmonary channels.
Semilunar valves • After formation of truncus septum (aorticopulmonary septum), three small tubercles or swellings appear in each of pulmonary and aortic channels. • The tubercles hollow out at their upper surfaces, forming Semilunar valves. • Neural crest cells contribute to these tubercles.
Formation of the muscular interventricular septum • During 4th week muscular part of interventricular septum extends upwards from the floor of the primitive ventricle • - Interventricular foramen is a space between the upper part of the interventricular septum and the septum intermedium Septum intermedium
Septum Formation in the Ventricles • Muscular part of IV septum • Formed by apposition and gradual fusion of medial walls of expanding ventricles due to continuous growth of myocardium outside and trabecula formation inside • Membranous part of IV septum • formed from: • Inferior endocardial cushion • Right bulbus swelling • L bulbus swelling
Development of valves: • I. Mitral & tricuspid valves: • - Atrioventricular cushions appear at the atrioventricular orifice. These cushions are, ventral& dorsal cushions. • - The 2 cushions grow towards each other, till they meet & fuse together in the middle of the orifice. • - As a result of this fusion, the single atrioventricular orifice will divides into two (right & left) orifices. • - The cushions will form the cusps of mitral & tricuspid orifices.