Download
1 / 77
800 likes | 920 Views
Explore the historical evolution and modern techniques of labour analgesia, from the era of obstetric anaesthesia to the latest evidence-based methods like neuraxial analgesia. Discover pharmacological and non-pharmacological approaches, including narcotics, intradermal water injections, acupuncture, and inhalational analgesia. Learn about randomized studies, patient-controlled analgesia, and the comparison of different analgesic agents. Unravel the importance of pain management during labor for maternal satisfaction and neonatal outcomes.

E N D
Labour analgesia Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics, PhD(physiology) Mahatma Gandhi Medical College and Research Institute, Puducherry, India
But what is history ?? • The era of obstetric anaesthesia began with James Young Simpson, when he administered ether to a woman with a deformed pelvis during childbirth. • His concept of “etherization of labour” was strongly condemned by critics • Religion condemned !!
1853, when John Snow administered chloroform to Britain’s Queen Victoria during the birth of her eighth child, Prince Leopold • In 1950 s – neuraxial techniques came into existence
The International Association for the Study of Pain (IASP) declared 2007–2008 as the • ’’Global Year against Pain in Women - Real Women, Real Pain.” • Still only 60 % accept or opt for epidurals in UK !!
Awareness of labour analgesia Not a single participant knew that the delivery is possible without suffering from labour pains; (1.5%) were of the opinion that it was impossible; 196 (98%) did not know whether it is possible or not. An equal number had no idea about labour analgesia • 200 rural pregnant women • Anaesthesia, Pain & Intensive Care
Do we need it ?? • Is there a necessity??
We need some form of labour analgesia • So we need it !!
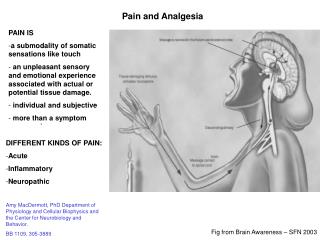
Visceral afferent pain fibers from the uterus, cervix, and upper vagina form the cervical plexus and enter the spinal cord at the T10–L1 levels. The visceral afferent fibers also enter the sympathetic chain at L2 and L3 levels. • lower vagina, vulva, and perineum. signals are conveyed via the S2–S4 spinal nerve roots that form the pudendal nerve
Hence a contradiction • First stage ---- T10 – L3 • Second stage --- S2, S3, S4
Now how to proceed • Give drugs – route ?? • Something other than drugs Pharmacological Non pharmacological
Non pharmacological • Lamaze in 1958 • The training starts from six weeks • During labour • Deep breath during contraction • Relax • Physician talks – electromyographic biofeedback with lamaze √ √ • Davidson hypnosis better than preparation alone
TENS • Four electrodes • Augustinson • 44% good relief 44 % acceptable 12 % nil
Acupuncture • Effective relief • Contractions become more regularized • Reduced oxytocin doses • But • wires • Time • Machinery • Interference with fetal monitoring ??
Position • Vertical position • Squatting – no proper studies • Ambulating ?? • Ambulating patients have shorter and less painful labour or vice versa ??
Intradermal Water Injections • The analgesic effect appears to last for 45 to 120minutes • reduce the rate of use of other analgesic techniques • Simple • No side effects
Some one may criticize ?? But no one stops a patient who is on intrathecal opioids to have hydrotherpay and intradermal water injection also Isnt it ??
Pharmacological • Narcotics • IM, SC or ( IV – more predictable, faster onset) • Pethidine – 1947 • The usual dose is 50 to 100 mg intramuscularly, which can be repeated every 4 hours. onset of analgesia occurs in 10 to 15 minutes, 45 minutes - reach peak effect. The duration -- 2 to 3 hours.
Other opioids • Morphine • Diamorphine • Meptazinol • Fentanyl , alfentanil, remifentanyl • Tramadol • Nalbuphine • Butorphanol • Pentazocine
Randomized studies • Significant relief • Easy to administer • Staff can manage • But studies reveal more percentage needed neonatal resuscitation ( morphine ?? ) • PCA - √ - better in less dosage , more analgesia and less side effects ( especially fentanyl)
A lot of studies • epidural analgesia is superior to remifentanil PCA, they also postulated that high maternal satisfaction with intravenous PCA may be the result of factors other than the degree of analgesia produced • What ? Is it so ?? • IV paracetomol • IV ketamine ( 0.2 mg/Kg) – 25 mg IV during crowning !!
Benzodiazepines ???? Analgesia ?? Amnesia !!
INHALATIONAL ANALGESIA • Nitrous oxide as premixed entonox 50 % • Separates at 7 degress c • Safety demand valve • Inhales at each contraction • Drowsy patient Stops • Effective . Crosses but safe to neonate • Equipment ?? • Resurgence of entonox !!
INHALATIONAL ANALGESIA- • Inhaled methoxyflurane with the help of a cardiff inhaler was practiced with conc. of 0.2 % • Enflurane • Isoflurane _ ? Less uterine atony • Sevoflurane – 0.7 MAC – good • Desflurane – cost and irritablity remains with efficiency less than nitrous oxide • Equipment, monitoring, aspiration risk , amnesia, timing ?? 0.5%MAC
Evidence based medicine • Systemic pethidine • Remifentanyl PCA • All agents in carefully monitored doses
Neuraxial analgesia • Spinal LA ? Opioids • Continuous epidural • CSEA • Caudal • Double catheter • Continuous spinal • Lumbar sympathetic ,paracervical • Pudendal ( nerve blocks )
Indications for epidural • Pre eclampsia/hypertensive disease • Prolonged labour • Two or more babies in utero • Anticipated instrumental delivery • Diabetes Mellitus • Breech presentation for vaginal delivery • Significant respiratory disease
Contraindications • No CTG tracing or inadequate CTG tracing e.g. loss of contact • Declined by the woman • Inadequate midwifery staffing levels. & • Otherwise similar as for other epidurals
Epidural technique • Prepare , position ,hydrate 500 ml of RL • Insert catheter – initiate dosage dilute local anaesthetics in 5 ml increments with lipid soluble opioid • TEST dose • Assess levels , monitor vitals • When ?? • Effective contractions 4 cm dilation in primi
Lidocaine, morphine, and meperidine are not commonly used for labor analgesia because of their short duration of action (lidocaine), long latency (morphine), and high incidence of nausea and vomiting (morphine and pethidine). Epidural block is the most effective and least depressant (pharmacologic option) allowing for an alert, participating mother
Opioids • Inadequate analgesics used alone • Synergistic with local anesthetics • Speedy onset of analgesia • Improves quality of analgesia • Permits use of very dilute LA solutions • Help relieve persistent perineal pain and unblocked segments
Intermittent • Epidural catch up phenomenon • Intermittent dose delayed • Severe pain • Influence the next dose
Infusion • Bupivacaine 10 ml /hour • Bupivacaine 12 ml/ hour with 2.5 mic/ml fentanyl • Ropivacaine 10 ml of 0.25 % • Levobupi + fentanyl • Lignocaine 0.75 %
Double catheter technique • Cleland • T11 catheter 6 ml of dilute solution of LA • Caudal catheter - 5 ml for stage 2
2 – 20 rule • Problem with neuraxialanaesthesia • 2 hour – dystocia in first stage • 20 min dystocia in second stage
CSEA • CSEA as a routine and are indicated only in certain specific situations, • like very early stage of labour where local anaesthetics are avoided, • advanced stages of labour where rapid analgesia is desirable • difficult epidurals as CSEA reduces the failure rate of epidurals.