Acute Coronary Syndrome Scorecard
The Acute Coronary Syndrome (ACS) Scorecard Tool is a comprehensive framework designed for healthcare providers to assess and enhance the performance of hospital care in relation to NQF-endorsed measures. It promotes quality improvement by identifying gaps and opportunities for better patient outcomes in ACS management. Users can evaluate solutions against specific performance measures and track them using the scorecard's data-driven approach. This tool aligns with the HCC Spectrum system, providing vital insights for improving acute coronary syndrome care.

Acute Coronary Syndrome Scorecard
E N D
Presentation Transcript
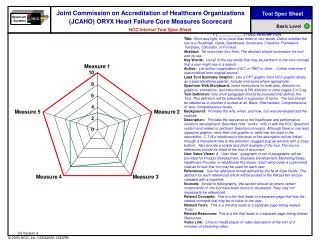
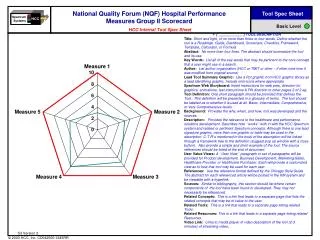
Spectrum Systems HCC National Quality Forum (NQF) Endorsed Voluntary Consensus Standards for Hospital Care: Acute Coronary Syndrome (ACS) Scorecard Tool Spec Sheet HCC Internal Tool Spec Sheet Basic Level • [ ____________ ] TOOL DESCRIPTION • Title: Short and tight, of no more than three or four words. Define whether the tool is a Roadmap, Guide, Dashboard, Scorecard, Checklist, Framework, Template, Calculator, or Formula. • Abstract: No more than four lines. The abstract should summarize the tool and its use. • Key Words: List all of the key words that may be pertinent to the core concept that a user might use in a search. • Author: List author organization (HCC or TMIT or other – if other note how it was modified from original source). • Lead Tool Summary Graphic:Use a PPT graphic from HCC graphic library as a lead identifying graphic. Include mini-icons where appropriate. • Spectrum Web Storyboard: Insert instructions for web pres, direction for graphics, animations, text instructions & PN direction to other pages 2 of 2 eg. • Tool Definition: One short paragraph should be provided that defines the Tool. This definition will be presented in a glossary of terms. The tool should be labeled as to whether it is used at all, Basic, Intermediate, Comprehensive, or Very Comprehensive levels. • Background: Provides the why, when, and how, tool was developed and the sources. • Description: Provides the relevance to the healthcare and performance solutions development. Describes how “works” with in with the HCC Spectrum system and related or pertinent Spectrum concepts. Although there is one lead signature graphic, more than one graphic or table may be used in the description. C-T-R’s mentioned in the body of the description will be linked through a framework tree to the definition (suggest pop up window with a close button). Also provide a simple and short example of the tool. The source references should be listed at the end of document. • User Value Views: A “User View” paragraph or set of paragraphs will be provided for Product Development, Business Development, Marketing/Sales, Healthcare Provider, or Healthcare Purchaser. Each will provide a customized view as to how that tool may be used for each user. • References: Use the reference format defined by the NLM Style Guide. The abstract for each referenced article will be posted in the KM system and be viewable with a hyperlink. • Sources: Similar to bibliography, this section should list where certain components of the tool have been found or developed. They may not necessarily be referenced. • Related Concepts: This is a link that leads to a separate page that lists the related concepts that may be of value to the user. • Related Tools: This is a link that leads to a separate page listing related Tools. • Related Resources: This is a link that leads to a separate page listing related Resources. • Video Link: Links to media player of video description of the tool (2-3 minutes) of streaming video. S3 Version 2
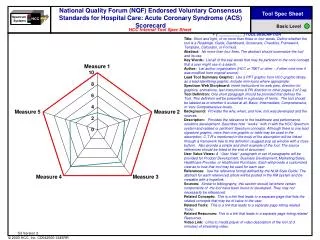
Spectrum Systems HCC National Quality Forum (NQF) Endorsed Voluntary Consensus Standards for Hospital Care: Acute Coronary Syndrome (ACS) Scorecard Tool Description Page 1 of 3 Basic Level • Related Concepts, Tools, and Resources: • Measures-Standards-Practices Grid • Performance M-S-P document • NQF Resource • Instructions: • The purpose of this tool is to evaluate the performance of the solution against specific NQF Measures-Standards-Practices and determine the opportunity gap. • Step 1: Review the definition of the Measures-Standards-Practices (select which) on the following page and determine if the solution has an impact on meeting, supporting, or providing data for the M-S-P. For more details refer to the M-S-P Tool. • Step 2: Click on Radar graph below and update the values using the scale 0-10 (10 being an exact match to fulfilling the measure). Use information as input data for the Index Model to determine specific Procedure volumes targeted by the solution. Notes and Comments: Completed by: Date: Version: Filing Location: S3 Version 2
Completed by: Filing Location: Version: Date: Spectrum Systems HCC Tool Template NQF-Endorsed Voluntary Consensus Standards: ACS Page 2 of 3 Basic Level S3 Version 2
Completed by: Filing Location: Version: Date: Spectrum Systems HCC Tool Template NQF-Endorsed Voluntary Consensus Standards: ACS Page 3 of 3 Basic Level • Acute Coronary Syndrome is the term given to any kind of myocardial ischemia, or blockage of blood flow to the heart. An individual who goes to the hospital with chest pain will be described in this way until further diagnosis has been performed. The result is usually angina or, in the most severe cases, infarction (heart attack). Rapid assessment usually involves an electrocardiogram, but in most cases Acute Coronary Syndrome is diagnosed as a chronic condition, based on history and risk factors. If left untreated, a heart attack is all but inevitable. • Definitions of the M-S-P: • Aspirin at arrival for acute myocardial infarction (AMI):Percentage of AMI patients who received aspirin within 24 hours before or after hospital arrival. Studies have demonstrated that AMI patients who receive aspirin shortly after hospital arrival suffer reductions in mortality and other adverse events by as much as 20%. Aspirin now plays a major role in the treatment and prevention of AMI in those who show early warning signs. • Aspirin prescribed at discharge for AMI:Percentage of AMI patients who were prescribed aspirin upon hospital discharge. Studies show that the long-term use of aspirin following AMI significantly reduces risks of additional heart attacks or strokes. JCAHO therefore recommends long-term aspirin therapy for all patients treated for AMI. • Beta Blocker at arrival for AMI:Percentage of AMI patients who received a beta blocker within 24 hours after hospital arrival. Beta blockers are any of a list of agents that act to slow heart rate and decrease contraction strength, thereby reducing blood pressure and oxygen usage. The immediate administering of beta blockers upon hospital arrival has shown to have the greatest effect on the prevention of AMI mortality, by reducing the magnitude of the infarction and all associated complications. Also, the earlier the beta blocker is administered, the less likely reinfarction will occur. • Beta Blocker prescribed at discharge for AMI:Percentage of AMI patients who were prescribed beta blockers upon hospital discharge. In spite of their well-documented benefits, beta blockers seem to be significantly under-utilized. Evidence shows that use of beta blockers following discharge significantly reduces the risk of further complications as a result of AMI. • AMI inpatient mortality:Percentage of AMI patients who expired during the hospital stay. Risk adjusted using JCAHO’s logistic regression model for ORYX measures. • Angiotensin converting enzyme inhibitor (ACEI) for left ventricular systolic dysfunction (LVSD):Percentage of AMI patients with LVSD who were prescribed ACEI at discharge. LVSD occurs when the contractile function of the left ventricle falls to below 40% of the standard performance rate. Angiotensin Converting Enzyme Inhibitors (ACEI) are a family of medicines that block the formation of angiotensin II, thereby reducing blood pressure. ACE Inhibitors prescribed to heart failure patients with LVSD have shown to significantly reduce recovery time, mortality rates, and re-hospitalization. • Percutaneous coronary intervention (PCI) within 120 minutes of arrival for AMI and Volume:Percentage of AMI patients who received PCI within 120 minutes of hospital arrival. PCI is any device that attempts to cross one or more coronary lesions, namely balloon angioplasty (PTCA), rotational, directional, or extraction atherectomy, laser angioplasty, or implantation of intracoronary stents or other catheter devices for treating coronary atherosclerosis. • Thrombolytic agent within 30 minutes of arrival for AMI:Percentage of AMI patients who received thrombolytic therapy within 30 minutes of hospital arrival. When a patient comes in suffering an AMI, it is imperative that blood flow be re-established as soon as possible. For certain kinds of infarctions, several new “clot-busting drugs,” collectively known as thrombolytic agents, can help dissolve blood clots and prevent heart damage, but only if they are administered in a timely manner. • Coronary Artery Bypass Graft (CABG) mortality:Percentage of isolated CABG surgery patients who died. Adjusted using New York State Cardiac Surgery Reporting System’s logistic regression model. CABG is the process of removing a clean blood vessel from the chest, arm, or leg, and re-attaching it elsewhere in order to re-route blood around a blocked artery. • CABG volume: Raw number of isolated CABG surgeries performed. • Coronary artery bypass graft (CABG) using internal mammary artery (IMA): Number of CABG patients who received an IMA graft. This surgery specifically involves the use of one of the blood vessels located on the inside of the chest cavity to re-route blood around a blocked artery. • PCI volume: Raw number of PCIs performed. • PCI mortality: Percentage of patients receiving PCIs who died. Adjusted using American College of Cardiology logistic regression model. S3 Version 2