Download
1 / 50
500 likes | 529 Views
Learn about increased intracranial pressure, its causes, symptoms, and complications. Explore Monro-Kellie doctrine, pathophysiology, signs, and diagnostic methods.

E N D
The pressure-volume relationship between ICP, volume of CSF, blood, and brain tissue, and cerebral perfusion pressure (CPP) is known as the Monro-Kellie doctrine or the Monro-Kellie hypothesis. The Monro-Kellie hypothesis
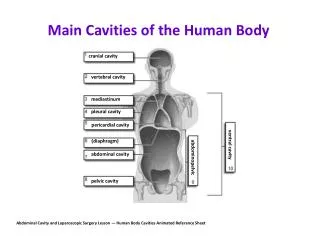
The Monro-Kellie hypothesis • The Monro-Kellie hypothesis states that the cranial compartment is incompressible, and the volume inside the cranium is a fixed volume. • The cranium and its constituents (blood, CSF, and brain tissue) create a state of volume equilibrium, such that any increase in volume of one of the cranial constituents must be compensated by a decrease in volume of another.
INCREASED ICP is a rise in the pressure inside the skull that can result from or cause brain injury. Or It is a life threatening situation that results from an increase in any or all of the 3 components (brain tissue, blood and CSF) of the skull. Definition
Causes of increased ICP include a rise in cerebrospinal fluid pressure, increased pressure within the brain matter, bleeding into the brain or fluid around the brain, or swelling within the brain matter itself.
Any lesion that increases one or more of the intracranial content is called a space occupying lesion. • Cerebral edema is one of the major cause. Conditions associated with cerebral edema are • Mass lesion • Head injury • Brain inflammation - Encephalitis, Meningitis • Aneurysm rupture Causes
Hydrocephalus • Bleeding in to the brain or spinal cord (Subdural hematoma, Subarachnoid hemorrhage and hematoma ) • Status epilepticus • Stroke • Lead and aresenic intoxication • Reye’s syndrome
Increased ICP from any cause decreases cerebral perfusion, stimulates further swelling (edema), and shifts brain tissue through openings in the rigid dura, resulting in brain herniation a frequently fatal event. Pathophysiology
Cerebral blood flow (CBF) is the amount of blood in milliliters passing through 100g of brain tissue in 1 min Normally CBF is approximately 50 mL per minute per 100 g of brain tissue White matter has a slower blood flow (25 ml/min/100g brain tissue) Gray matter -75ml/min/100gm brain tissue
The blood flow to the brain is that much critical because the brain requires a 20% of oxygen and 25% of glucose Inadequate perfusion leads to increase CO2 concentration
Behavior changes • Decreased consciousness, Lethargy, Seizures, back pain. • Vomiting – non projectile and without nausea • Headache - The headache is classically a morning headache which may wake them from sleep. The headache is worse on coughing / sneezing / bending, and progressively worsens over time • Neurological symptoms, including weakness, numbness, eye movement problems, and double vision Signs and symptoms
Occular problmes Compression of occulomotor nerve results in - Dilation of pupil Sluggish or no response to light Inability to move the eye upward Ptosis of the eye lid Papilledema (swelling of optic disc) -it may lead to visual disturbances, and eventually blindness.
Changes in vitals – increased BP and altered respiration • If brain tissues displaced - Cushing's triad involves an increased systolic blood pressure, bradycardia, and an abnormal respiratory pattern. • Cheyne–Stokes respiration, in which breathing is rapid for a period and then absent for a period
Altered Motor function – hemiparesis or hemiplegia Decorticate posture or decorticate response Flexion of arms, wrist and fingers with adduction in upper extremity Extension, internal rotation of plantar flexion in lower extremity Decerebrate posture/ decerebrate responses All four extremities in rigid extension with hyper pronation of forearm , adduction of upper extremity, flexion of wirst with plantar flexion of feet
Opisthotonic posturing – a muslce spasm causing the back to be arched to the head retracted, with great rigidity of the muscle of the neck and back.
Restlessness (without apparent cause), confusion, or increasing drowsiness As ICP increases, the patient becomes stuporous, reacting only to loud auditory or painful stimuli In severe increase, exceeds 40-50mm hg - comatose When the coma is profound, death is inevitable.
History and Physical examination Vital sign, neurological assessment Skull, chest and spinal x ray cerebral angiography, computed tomography (CT) scanning, or magnetic resonance imaging (MRI). PET SCAN, EEG, ECG Transcranial Doppler studies provide information about cerebral blood flow. Lumbar puncture is avoided in patients with increased ICP because the sudden release of pressure can cause the brain to herniate. Assessment and Diagnostic Findings
CBC Coagulation profile Electrolytes, ABG’S, toxicology screen CSF analysis for protein, cells, glucose
ICP MEASUREMENTS Intracranial pressure monitoring is performed by inserting a catheter into the head with a sensing device to monitor the pressure around the brain.
ICP Monitoring Devices Location • Ventricular • Parenchymal, Epidural • Subarachnoid, Subdural Product catheter with drainage Codman, Camino Bolt system
CSF drainage Ventriculostomy – gold standard procedure • A catheter is inserted into the lateral ventricle using a closed system. • The 3 way stopcock is opened to allow CSF to flow into the draining bag (30 – 120 sec) Advantages • Directly measure the pressure with in the ventricle • Facilitate removal and sampling of CSF • Allows intra ventricular drug administration
HOB elevated 30° ↑ venous drainage Head midline↑ venous drainage No jugular catheters prevent venous obstruction Normothermiaavoid ↑ metabolism General Care
Medical Management • Maintaining oxygenation • Invasive ICP monitoring • Decreasing cerebral edema • Maintaining cerebral perfusion • Lowering CSF volume • Controlling fever • Reducing metabolic demands
Increased ICP is a true emergency and must be treated immediately through: a. Maintaining oxygenation: • Intubation and mechanical ventilation • ABG analysis • Elevation of head of the bed to 30 degree with head in a neutral position b. Invasive monitoring of ICP • to identify increased pressure • the degree of elevation • to initiate appropriate treatment • to provide access to CSF for sampling and drainage • to evaluate the effectiveness of treatment.
c. Decreasing cerebral edema: • Osmotic diuretics (mannitol) - given to dehydrate the brain tissue and reduce cerebral edema. They reduce the volume of brain and extracellular fluid • Loop diuretics (frusimide) • Cortico steroids (dexamethasone) – help to reduce cerebral edema when a brain tumor is the cause of increased ICP.
d. Maintaining cerebral perfusion: • The cardiac output may be manipulated to provide adequate perfusion to the brain. • Inotropic agents such as dobutamine hydrochloride are used. • A lower cerebral perfusion pressure indicates that the cardiac output is insufficient to maintain adequate cerebral perfusion. • Cerebral perfusion pressure (CPP) is defined as the difference between mean arterial and intracranial pressures. Mean arterial pressure is the diastolic pressure plus one third of the pulse pressure (difference between the systolic and diastolic). MAP is thus between systolic and diastolic pressures. • CPP = MAP(70 -110 mmhg) – ICP(0-15 mmhg) • Normal cerebral perfusion pressure is 60-80 mmHg, nearer diastolic.
e. Lowering the volume of CSF and cerebral blood: • CSF drainage is frequently performed because the removal of CSF with a ventriculostomy drain may dramatically reduce ICP and restore cerebral perfusion pressure. f. Controlling fever: • Preventing a temperature elevation is critical because fever increases cerebral metabolism. • Antipyretics • Cold applications .
g. Reducing metabolic demands: • Barbiturates (sedatives) -Cellular metabolic demands can be reduced (high doses). • Barbiturates induce coma, lower ICP and decrease mortality.
Drug therapy (drugs used in INCREASED ICP) • Osmotic diuretics • Loop diuretics • Corticosteroids • Barbiturates • Ionotropic drugs • Sedatives • Paralazing drugs • Analgesics • Antiseizure drugs
Nutritional therapy • Nutritional replacements should begins within 3 days after injury. • Patient is in hypermetabolic and hypercatabolic state • Need for glucose • Keep patient normovolemic • IV 0.45% or 0.9% sodium chloride
Opening in the cranium for access to brain • As raised ICP's may be caused by the presence of a mass, removal of this via craniotomy will decrease raised ICP's. • A drastic treatment for increased ICP is decompressivecraniectomy, in which a part of the skull is removed and the dura mater is expanded to allow the brain to swell without crushing it or causing herniation. • The section of bone removed, known as a bone flap, can be stored in the patient's abdomen or thigh and resited back to complete the skull. • Alternatively a synthetic material may be used to replace the removed bone section Craniotomy
Methods are provided for preserving and restoring cranial bone flaps. In one aspect, the method to preserve a cranial bone flap includes cleaning a cranial bone flap, washing the cranial bone flap with a sterile saline solution including gentamycin, and washing the bone with a sterile saline solution including vancomycin. The cranial bone flap may be dried, wrapped, and packaged before being stored in a freezer.
The fixing method may include removing the preserved cranial bone flap from a freezer and unwrapping the preserved cranial bone flap from any wrappings. The preserved cranial bone flap may be washed with a sterile saline solution including gentamycin and a sterile saline solution including vancomycin.
Assessment: • Obtain a history of events leading to the present illness • The neurologic examination should include an evaluation of mental status, level of consciousness (LOC), cranial nerve function, cerebellar function (balance and coordination), reflexes, and motor and sensory function. Assessment of LOC includes eye opening; verbal and motor responses; pupils (size, equality, reaction to light). • Glasgow Coma Scale Nursing management
Eye opening response Spontaneous 4 To voice 3 To pain 2 None 1 Best verbal response Oriented 5 Confused 4 Inappropriate words 3 Incomprehensible sounds 2 None 1 Best motor response Obeys command 6 Localizes pain 5 Withdraws 4 Flexion (decorticate) 3 Extension (decerebrate) 2 None 1 Total 15 Glasgow Coma Scale
Nursing diagnoses: • Increased intracranial pressure assosiated with head injury • Ineffective airway clearance related to diminished protective reflexes (cough, gag) • Ineffective breathing patterns related to neurologic dysfunction • Ineffective cerebral tissue perfusion related to the effects of increased ICP • Risk for fluid and electrolyte imbalance related to osmotic diuretic therapy • Risk for physiologic injury related to seizures • Risk for infection related to altered nutrition
Nursing Interventions: • Maintaining patent airway. • Assess the patency of the airway. • Suction with care- secretions obstructing the airway, because transient elevations of ICP occur with suctioning. • The patient is hyperoxygenated before and after suctioning to maintain adequate oxygenation. • Discourage coughing because it increases ICP. • Auscultate the lung fields at least every 8 hours to determine the presence of abnormal breath sounds. • Elevate the head of the bed may aid in clearing secretions as well as improving venous drainage of the brain.
Achieving an adequate breathing pattern • Monitor the patient constantly for respiratory irregularities. This includes Cheyne-Stokes respirations (alternating periods of hyperpnea and apnea)
Monitor PaCO2 (normal range 35 to 45 mm Hg) if hyperventilation therapy has been decided to reduce ICP • Maintain a neurologic observation record. Repeated assessments of the patient are made frequently to immediately note improvement or deterioration.
Optimising cerebral tissue perfusion • Maintain head alignment and elevate head of bed 30 degrees. The rationale is that hyperextension, rotation, or hyperflexion of the neck causes decreased venous return. • Avoid extreme hip flexion as this increases intra-abdominal and intrathoracic pressures, leading to rise in ICP. • Avoid the Valsalva maneuver (straining at stool) as it raises ICP. Administer stool softeners as prescribed. If appropriate, provide high fiber diet. • Note abdominal distention. Avoid enemas
When moving or being turned in bed, instruct the patient to exhale to avoid the Valsalva maneuver. • If the patient is on mechanical ventilation, preoxygenate and hyperventilate him, before suction, using 100% oxygen on the ventilator. Suctioning should not last longer than 15 seconds. • Avoid activities that raise ICP if possible. Space nursing interventions; this may prevent transient increases in ICP.
During nursing interventions, the ICP should not rise above 25 mm Hg and should return to baseline levels within 5 minutes. • Patients with the potential for a significant increase in ICP should receive sedation or “paralyzation” before initiation of many nursing activities. • Avoid emotional stress, disturbances from sleep, and environmental stimuli (noise, conversation). • Isometric muscle contractions (Pushing against an immovable wall) are also contraindicated because they raise the systemic blood pressure and hence the ICP.
Inadequate cerebral perfusion • Cerebral herniation • Transforaminalherniation – occurs when the brainstem is forced downward through the foramen magnum • Uncalherniation – occurs when uncal portion of the temporal lobes shift over the edge of the tentoriumcerebelli • Cingulateherniation –brain is forced under the falx-cerebri that separates the cerebral hemispheres Complications