Download
1 / 76
760 likes | 799 Views
Explore the intricate structure and function of female breasts, from the mammary glands to lymphatic drainage, and how factors like genetics and diet influence size and shape. Learn about the vasculature of the breast and the importance of lymphatic drainage for breast health.

E N D
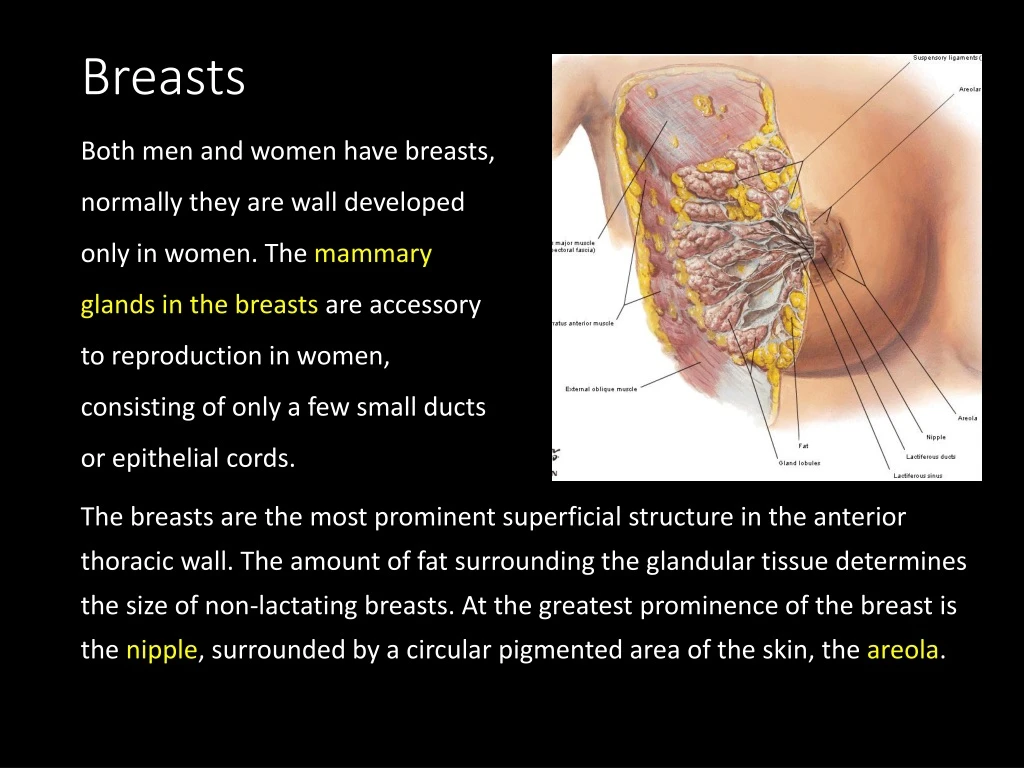
Breasts Both men and women have breasts, normally they are wall developed only in women. The mammary glands in the breasts are accessory to reproduction in women, consisting of only a few small ducts or epithelial cords. The breasts are the most prominent superficial structure in the anterior thoracic wall. The amount of fat surrounding the glandular tissue determines the size of non-lactating breasts. At the greatest prominence of the breast is the nipple, surrounded by a circular pigmented area of the skin, the areola.
Female breasts The female breast rests on a bed that extends transversely from the lateral border of the sternum to the midaxillary line and vertically from the 2nd through 6th ribs. Two thirds of the bed of the breast are formed by the pectoral fascia overling the pectoralis major; the other third, by the fascia covering the serratus anterior.
Female breasts Between the breast and the pectoral fascia is a loose connective tissue plane or potential space, the retromammary space. This plane, containing a small amount of fat. (boob job)
Female breasts The mammary gland is firmly attached to the dermis of the overlying skin, especially by substantial skin ligaments, the suspensory ligaments (of Cooper). Larger dimples (fingertip size or bigger) result from cancerous invasion of the glandular tissue and fibrosis (fibrous degeneration), which causes shortening or places traction on the suspensory ligaments.
Female breasts Breast size and shape are determined by genetic, ethnic, and dietary factors. The lactiferous ducts give rise to buds that form 15-20 lobules of glandular tissue, which constitute the parenchyma of the mammary gland. Each lobule is drained by a lactiferous duct, which usually opens independently on the nipple. The mammary glands are modified sweat glands; therefore, they have no special capsule or sheath. The rounded contour and most of the volume of the breasts are produced by subcutaneous fat.
Vasculature of the breast • Medial mammary braches of perforating branches and anterior intercostal branches of the internal thoracic artery • Lateral thoracic and thoracoacromial arteries, branches of the axillary artery. • Posterior intercostal arteries, branches of the thoracic aorta in the 2nd, 3rd, and 4th intercostal spaces.
The lymphatic drainage of the breast Most lymph (> 75%), especially from the lateral breast quadrants, drains to the axillary lymph nodes, initially to the anterior or pectoral nodes for the most part. However, some lymph may drain directly to other axillary nodes or deep cervical nodes.
The lymphatic drainage of the breast • Most of the remaining lymph, particularly from the medial breast quadrants, drains to the parasternal lymph nodes or the opposite breast, whereas lymph from the inferior quadrants may pass deep to abdominal lymph nodes. • Lymph from the skin of breast, drains into the ipsilateral axillary, inferior deep cervical, and infraclavicular lymph nodes, and also into the parasternal lymph nodes of the both sides.
Lungs The lungs are the vital organs of respiration. Their main function is to oxygenate the blood by bringing inspired air into close relation with the venous blood in the pulmonary capillaries. Although cadaveric lungs may be shrunken, firm or hard to the touch, and discolored in appearance, healthy lungs in living people are normally light, soft, and spongy, and fully occupy the pulmonary cavities. They are also elastic and recoil to approximately one third their size when the thoracic cavity is opened.
Root of Lungs The lungs are separated from each other by the mediastinum, to which they are attached by the roots of the lungs, that is the bronchi, pulmonary arteries, superior and inferior pulmonary veins, the pulmonary plexuses of nerves (sympathetic, parasympathetic, and visceral afferent fibers), and lymphatic vessels.
Hilum of the lungs Medial to the hilum, the root is enclosed within the area of continuity between the parietal and the visceral layers of pleura, the pleural sleeve, or mesopneumonium (mesentery of the lung), the hilum of the lung is a wedge-shaped area of the medial surface of each lung, the point at which the structures forming the root enter and leave the lung. The hilum can be likened to the area of earth where a plant’s roots enter the ground.
Lobes of the lungs The horizontal and oblique fissures divide the lungs into lobes. The right lung has three lobes, the left lung has two. The anterior border of the right lung is relatively straight, whereas this border of the left lung has a deep cardiac notch, an indentation consequent to the deviation of the apex of the heart to the left side. This indentation often creates a thin, tongue-like process of the superior lobe, the lingula.
Lungs • An apex, the blunt superior end of the lung ascending above the level of the 1st rib into the root of the neck that is covered by cervical pleura. • Three surfaces, costal, mediastinal, and disphragmatic. • Three border, anterior, inferior, posterior
Lungs The mediastinal surface of the lung includes the hilum and thus receives the root of the lung, around which the pleura forms the pleura sleeve. The pulmonary ligament hangs inferiorly from the pleural sleeve around the lung root. The diaphragmatic surface of the lung, forms the base of the lung, which rests on the dome of the diaphragm. Laterally and posteriorly, the diaphragmatic surface is bounded by a thin, sharp margin that projects into the costodiaphragmatic recess of the pleura. The anterior border of the lung is where the costal and medianstinal surface meet anteriorly and overlap the heart; the cardiac notch indents this border of the left lung.
Trachea and bronchi Beginning at the larynx, the walls of the airway are supported by horseshoe- or C-shaped rings of hyaline cartilage. The sublaryngeal airway constitutes the tracheobronchieal tree. The trachea, located within the superior mediastinum, and bifurcates at the level of the sternal angle into main (primary) brochi, one to each lung, passing inferolaterally to enter the lungs at the hila (hilum).
Main bronchus • The right main bronchus is wider, shorter, and runs more vertically the the left main bronchus as it passes directly to the hilum of the lung. • The left main bronchus passes inferolaterally, inferior to the arch of the aorta and anterior to the esophagus and thoracic aorta, to reach the hilum of the lung.
Bronchi branch Within the lung, the bronchi branch in a constant fashion to form the roots of the tracheobronchial tree, as components of the root of the each lung. Each main bronchus divides into lobar bronchi (secondary bronchi), two on the left and three on the right, each of which supplies a lobe of the lung. Each lobar bronchus divides into several segmental bronchi (tertiary bronchi) that supply the bronchopulmonary segment.
Bronchopulmonary segments • Pyramidal-shaped segments of the lung, with their apices facing the lung root and their bases at the pleural surface. • The largest subdivision of a lobe. • Separated from adjacent segments by connective tissue septa. • Supplied independently by a segmental bronchus and tertiary branch of the pulmonary artery.
Bronchopulmonary segments • Named according to the segmental bronchi supplying them. • Drained by intersegmental parts of the pulmonary veins that lie in the connective tissue between and drain adjacent segments. • Surgically resectable. • Usually 18-20 in number (10 in the right lung 8-10 in the left lung).
Bronchopulmonary segments • Beyond the direct branches of the lobar bronchi – that is, beyond the segmental bronchi – are from 20 to 25 generations of branches that eventually end in terminal bronchioles.
Bronchopulmonary segments • Each terminal bronchioles gives rise to several generations of respiratory bronchioles, and each respiratory bronchiole provide 2-11 alveolar ducts, each of which gives rise to 5-6 alveolar sac lined by alveoli. The pulmonary alveolus is the basic structure unit of gas exchange in the lung.
Mediastinum The mediastinum, occupied by the mass of tissue between the two pulmonary cavities, is the central compartment of the thoracic cavity. It is covered on each side by mediastinal pleura and contains all the thoracic viscera and structures except the lungs.
Mediastinum The mediastinum is artificially divided into superior and inferior parts for purposes of description. The superior mediastinum extends inferiorly from the superior thoracic aperture to the horizontal plane that includes the sternal angle anteriorly and passes approximately through the junction (IV disc) of the T4 and T5 vertebrae posteriorly, often referred to the transverse thoracic plane. Inferior mediastinum, between this plane and the diaphragm, is further subdivided by the pericardium into anterior, middle, and posterior parts. The pericardium and its contents (the heart and roots of the its great vessels) constitute the middle mediastinum.
Pericardium The middle mediastinum includes the pericardium, heart, and roots of its great vessels, ascending aorta, pulmonary trunk, and SVC, passing to and from the heart. The pericardium is a fibroserous membrane that covers the heart and the beginning of its great vessels. The pericardium is a closed sac composed of two layer. The tough external layer, the fibrous pericardium, is continuous with the central tendon of the diaphragm. The internal surface of the fibrous pericardium is lined with a glistening serous membrane, the parietal layer of serous pericardium.
Pericardium The middle mediastinum includes the pericardium, heart, and roots of its great vessels, ascending aorta, pulmonary trunk, and SVC, passing to and from the heart. The pericardium is a fibroserous membrane that covers the heart and the beginning of its great vessels. The pericardium is a closed sac composed of two layer. The tough external layer, the fibrous pericardium, is continuous with the central tendon of the diaphragm. The internal surface of the fibrous pericardium is lined with a glistening serous membrane, the parietal layer of serous pericardium.
Pericardium This layer is reflected onto the heart at the great vessels- aorta, pulmonary trunk and vein, and superior and inferior venae cavae - as the visceral layer of the serous pericardium. The serous pericardium, is a single layer of the flattened cells forming an epithelium that lines both the internal surface of the fibrous pericardium and the external surface of the heart.
Pericardium The fibrous pericardium is • Continuous superiorly with the tunica adventitia of the great vessels. • Attached anteriorly to the posterior surface of the sternum by the sternopericardial ligament. • Continuous inferiorly by with the central tendon of the diaphragm. • Bound posteriorly by loose connective tissue to structures in the posterior mediastinum.
Heart General descrption 1. Larger than a clenched fist 2. Double, self-adjusting muscular pump 3. Weight 280-340 gm in men 230-280 gm in women
4. The heart has four chambers Atrium is a receiving area that pumps blood into a ventricle(a discharging chamber)
5. The wall of each chamber consists of three layers Internal layer (endocardium), endothelium and subendothelial connective tissue. Middle layer (myocardium composed of cardiac muscle which forms the main mass of the heart) External layer (epicardium), formed by the visceral layer of serous pericardium.
The heart and roots of the great vessles within the pericardial sac are related anteriorly to the seternum, costal cartilages, and anterior ends of the 3rd-5th ribs on the left side. The heart and pericardial sac are situated obliquely, approximately two thirds to the left and one third to the right of the median plane.
6. The heart has a base (posterior aspect), apex (inferolateral end), three surfaces (sternocostal, diaphragmatic, and pulmonary), and four borders (right, inferior, left, and superior). The base of the heart the base is located posteriorly and is formed mainly by the left atrium, faces posteriorly toward the bodies of vertebrae T5-T8 (supine) /T6-T9 (erect) . Extends superiorly to the bifurcation of the pulmonary trunk and inferiorly to the coronary groove.
The apex of the heart the blunt apex is formed by the left ventricle, which points inferolaterally. It is located posterior to the left fifth intercostal space in adults, 7 to 9 cm from the median plane and just medial to the left midclavicular line. The apex beat is an impulse imparted by the heart, it is its point of maximal pulsation.
Sternocostal surface, formed mainly by the right ventricle and is visible in radiographs of the thorax. Diaphragmatic (inferior) surface, is usually horizontal or slightly concave. It is formed by both ventricles, mainly the left one. This surface is related to the central tendon of the diaphragm. The posterior interventricular groove divides this surface into a right one-third and a left two-thirds.
The borders of the heart Right border, formed by the right atrium and extending between the SVC and the IVC. Inferior border, which is sharp and thin, is nearly horizontal. It is formed mainly by the right ventricle and only slightly by the left ventricle. Left border is formed mainly by the left ventricle and only slightly by the left auricle. Superior border is where the great vessels enter and leave the heart. It is formed by the right and left auricles with the superior conical portion of the right ventricles, the conusarteriosus (infundibulum), between them. The pulmonary trunk arises from the conusarteriosus.
Chambers of the heart The heart has four chambers, two atria and two ventricles.
The coronary groove (sulcus) encircles most of the superior part of the heart and separates the atria form the ventricles. Similarly, division of the ventricles is indicated by the anterior and posterior interventricular grooves (sulci)
Right Atrium • This chamber forms the right border of the heart between the SVC, IVC. It receives venous blood from these large vessels and the coronary sinus. • The interior of the right atrium has a : • Smooth posterior part, (the sinus venarum, or sinus of the venae cavae), which reveives the venae cavae and coronary sinus. • Rough, muscular anterior wall composed of pectinate muscles.
The right auricle (atrial appendage) is a small , conical muscular pouch that projects to the left from the right atrium and overlaps the ascending aorta. The two distinct parts of the right atrium are separated externally by a shallow vertical groove on the posterior aspect of the right atrium, the sulcus terminalis and internally by a vertical ridge, the crista terminalis. The crista extends between the two vena caval orifices.
The smooth and rough parts of the atrial wall are separated externally by a shallow vertical groove, the sulcus terminalis or terminal groove, and internally by a vertical ridge, the crista terminalis or terminal crest. The SVC opens into the superior part of the right atrium at the level of the right 3rd costal cartilage. The IVC opens into the inferior part of the right atrium at the level of the 5th costal cartilage. The opening of the coronary sinus, a short venous trunk receiving most of the cardiac veins, is between the right AV orifice and the IVC orifice. The interatrial septumseparating the atria has an oval, thumbprint-size depression, the oval fossa, which is a remnant of the oval foramen and its valve in the fetus.
Superior vena cava (SVC), returing blood from the superior half of the body, opens into the superoposterior part of the right atrium. Its orifice, usually valveless, is directed inferoanteriorly. Inferior vena cava (IVC), returing blood from the inferior half of the body, opens into the inferior part of the right atrium. The rudimentary valve of IVC is a thin fold of variable size that connects the anterior margin of its orifice to the anterior part of the limbus fossae ovalis. This valve is nonfunctional after birth.
Right ventricle The right ventricle forms the largest part of the sternocostal (anterior) surface of the heart, a small part of the diaphragmatic surface, and almost the entire inferior border of the heart. Its superior left angle tapers into a cone-shaped pouch, the infundibulum or conus arteriosus, which leads into the pulmonary trunk. The interior of the right ventricle has irregular muscular elevations (trabeculae carneae). A thick muscular ridge, the supraventricular crest, separates the ridged muscular wall of the inflow partof the chamber from the smooth wall of the conus arteriosus, or outflow part.
The inflow part of the ventricle receives blood from the right atrium through the right AV (tricuspid) orifice, located posterior to the sternum at the level of the 4th and 5th intercostal spaces. The right AV orifice is surrounded by one of the fibrous rings of the fibrous skeleton of the heart. The fibrous ring keeps the caliber of the orifice constant, resisting the dilation that might otherwise result from blood being forced through it at varying pressures.
The tricuspid valve guards the right AV orifice. The bases of the valve cusps are attached to the fibrous ring around the orifice. Because the fibrous ring maintains the caliber of the orifice, the attached valve cusps contact each other in the same way with each heartbeat. Tendinous cordsattach to the free edge and ventricular surfaces to the anterior, posterior, and septal cusps, much like the cords attaching to a parachute. The tendinous cords arise from the apices of papillary muscles, which are conical muscular projections with bases attached to the ventricular wall.
The papillary muscles begin to contract before contraction of the right ventricle, tightening the tendinous cords and drawing the cusps together. Because the cords are attached to adjacent sides of two cusps, they prevent separation of the cusps and their inversion when tension is applied to the tendinous cords and maintained throughout ventricular contraction (systole), that is the cusps of the tricuspid valve are prevented from prolapsing as ventricular pressure rises. Thus regurgitation of blood from the right ventricle back into the right atrium is blocked by the valve cusps.
Three papillary muscles in the right ventricle correspond to the cusps of the tricuspid valve: The anterior papillary muscle, the largest and most prominent of the three, arises from the anterior wall of the right ventricle, its tendinous cords attach to the anterior and posterior cusps of the tricuspid valve. The posterior papillary muscle, may consist of several parts, it arises from the inferior wall of the right ventricle, and its tendinous cords attach to the posterior and septal cusps of the tricuspid valve. The septal papillary muscle, arises from the interventricular septum, and its tendinous cords attach to the anterior and septal cusps of the tricuspid valve.
Theinterventricular septum (IVS), composed of muscular and membranousparts, is a strong, obliquely placed partition between the right and left ventricles, forming part of the walls of each. Because of the much higher blood pressure in the left ventricle, the muscular part of the IVS, which forms the majority of the septum. Superiorly and posteriorly, a thin membrane, part of the fibrous skeleton of the heart, forms the much smaller membranous part of the IVS. On the right side, the septal cusp of the tricuspid valve is attached to the middle of this membranous part of the fibrous skeleton. This means that inferior to the cusp the membrane is an interventricular septum, but superior to the cusp it is an atrioventricular septum, separating the right atrium from the left ventricle.
The septomarginal trabecula(moderator band) is a curved muscular bundle that transverse the right ventricular chamber from the inferior part of the IVS to the base of the anterior papillary muscle. This trabecula is important because it carries part of the right branch of the AV bundle, a part of the conducting system of the heart to the anterior papillary muscle.
The right atrium contracts when the right ventricle is empty and relaxed; thus blood is forced through this orifice into the right ventricle, pushing the cusps of the tricuspid valve aside like curtains. The inflow of blood into the right ventricle (inflow tract) enters posteriorly; and when the ventricle contracts, the outflow of blood into the pulmonary trunk (outflow tract) leaves superiorly and to the left. The pulmonary valve at the apex of the conus ateriosus is at the level of the left 3rd costal cartilage.