Download
1 / 64
690 likes | 1.11k Views
DIAGNOSIS OF CARDIAC RHYTHMS. Lecture #2. I. Common Terminology. Supraventricular vs. Ventricular Rhythms • The differential is made on the basis of QRS duration • If the QRS complex is narrow (< 0.12 sec): – T he ventricular myocardium is depolarized rapidly

E N D
DIAGNOSIS OFCARDIAC RHYTHMS Lecture #2
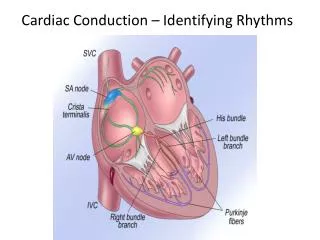
I. Common Terminology Supraventricular vs. Ventricular Rhythms • The differential is made on the basis of QRS duration • If the QRS complex is narrow (< 0.12 sec): – The ventricular myocardium is depolarized rapidly – The rhythm is supraventricular in origin • If the QRS complex is wide (> 0.12 sec): – There is a delay in the spread of the electrical activation throughout the ventricles – The origin of the rhythm may be in the ventricle itself
Premature Atrial Contraction (PAC) • P-waves differ from normal • P-waves appear early • P-waves are followed by a normal-appearing QRS complex
Premature Ventricular Contraction (PVC) • NO P-waves present • QRS complex is wide • Ventricular Tachycardia (VT) 3 consecutive PVC’s, at a rate 100 bpm (Non-sustained VT - <30 sec)
I. Common Terminology (cont’d) Arrhythmia • Generally referred to as any rhythm other than normal sinus rhythm 3 general mechanisms that can cause arrhythmias: Disorders of impulse formation: • Altered Automaticity • Triggered activity Disorders of impulse conduction: 3. Re-entry
Mechanism of Arrhythmias: Re-entrant Tachycardia • Rhythm is secondary to a “loop” in the electrical circuitry (the re-entry pathway) resulting in tachycardia • Requires: • Unidirectional block (with recovery) • Slowed conduction through loop • It may occur within the SA node, the AV node, or actually any ectopic foci in the atria or ventricles
1. Sinus Rhythm • Normal Sinus Rhythm • Rate = 60 – 99 bpm • Sinus Bradycardia • Rate 59 bpm • Sinus Tachycardia • Rate 100 bpm
Sinus Rhythm Criteria: 1. Every QRS complex is precededby a P-wave 2. P-waves appear normal, that is they are ofsinus node origin: A. Normal Morphology: 1. P-wave duration < 0.12 sec (< 3 boxes) 2. P-wave height < 2.5 mm (< 2.5 boxes) B. Normal Axis: 1. P-waves is upright in leads II, III & aVF 2. P-waves is negative in leadaVR
2. Paroxysmal Atrial Tachycardia (PAT) • Re-entrant tachycardia of supraventricular origin, with a rate of 120 – 180 bpm (narrow complex) • P-waves may or may not be visible, depending on the rate • If present, P-waves are usually regular and inverted in lead II (they may be seen before, during, or after the QRS complexes) • Usually idiopathic, but can also be seen in RHD, COPD, MVP & digitalis toxicity
3. Atrial Flutter A. Atrial rate ~ 250 – 350 bpm B. Characterized by rapid, undulating“flutter-waves”: 1. Are best seen in leads aVF & V1 2. Have a longer duration & a greater amplitude than a normal P-wave 3. Have a saw-toothed appearance C. There is always some degree of AV-block present (2:1, 3:1 or variable), which is why the atrial rate is always much greater than the ventricular rate
Atrial Flutter (cont’d) D. Carotid sinus massage– may exaggerate the degree of AV-block & consequently slow down the QRS rate, to assist with the diagnosis – This makes the flutter-waves more obvious!
4. Junctional Rhythm A. Impulses originate in theAV node with retrograde & antegrade conduction B. QRS complexes are narrow & regular (this is still considered supraventricular!) C. P-waves may be inverted in leads II, III & aVF & may occur before, duringorafter the QRS complexes D. Junctional Rate = 40 – 55 bpm E. This is usually an escape rhythm due to SA node dysfunction ordigitalis toxicity!
AV-Nodal Re-entrant Tachycardia (AVNRT) • One of the most common causes of PSVT • P-waves may not be visible or may occur before, during or after the QRS complexes • Two pathways usually exist: slow (anterograde conduction) & fast (retrograde conduction) D. More common in younger patients E. Abrupt onset & offset
6. AV Re-entrant Tachycardia (AVRT) • Another common cause of PSVT • Involves an “accessory pathway” (1:1500) • Usually utilizes the AV node as the anterograde & the accessory pathway as the retrograde limbs (Orthodromic AVRT) – accessory pathway may be “concealed” • In 10%, impulse travels retrograde across AVN, and anterograde over accessory pathway (Antidromic AVRT) – “pre-excitation” present
Pre-excitation Pre-excitation: Impulse travels anterogradely th’ AV node + accessory pathway to ventricles Examples include pre-excitation syndromes: – Wolff–Parkinson–White syndrome (pre-excitation + tacchycardia) – Lown-Ganong-Levine (LGL) syndrome – “Mahaim fiber tachycardias”
Wolff–Parkinson–White (WPW) A. A supraventricular rhythm originating in the SA node with normal & regular P-waves B. PR interval is abnormally short (< 0.12 sec) C. QRS is wide with a “slurred upstroke” (AKA thedelta-wave) • Delta-waves are due to the accessory conduction pathway (bundle of Kent) from the atria to the ventricles, that bypasses the AV node • Must manifest a tacchycardia at some point in time E. Rx: Procainamide
2. Wandering Atrial Pacemaker (WAP) A. Pacing is from various foci within the atria B. Heart rate <100 bpm C. Contour or shape of P-waves vary from beat to beat, in a single lead (always try to look at lead II!) • Associated with variations of P-R & P-P intervals, resulting in an irregularly irregular rhythm E. A common cause is rheumatic heart disease • So, Dx Criterion: Three consecutive P-waves with different morphologies, on a single EKG lead, with a heart rate <100 bpm
3. Multifocal Atrial Tachycardia (MAT) A. Multifocal Atrial Tachycardia (MAT) is similar to wandering atrial pacemaker, except that the heart rate 100 bpm • Again, you must have three different consecutive P-wave morphologies on a given lead (again, examine lead II!) C. Irregularly irregular rhythm D. Usually associated with end-stage COPD E. Rx: Control the rate & treat the underlying problem
4. Atrial Fibrillation A. Random chaotic depolarizations of the atria at rates > 300 bpm B. NO effective pumping of the atria takes place – You loose ~25% of C.O., AKA the “atrial kick” C. Irregularly irregular rhythm • May occur in any clinical situation which causes LAE, hyperthyroidism, or also with EtOH use (“holiday heart”) E. Rx: Rate control & anti-coagulation
Atrial Fibrillation • The ventricular rate can be either rapid or well-controlled, depending on the conduction through the AV node
1. Idioventricular Rhythms • Rhythm originates in the ventricles, giving rise to wide& bizarreQRS complexes B. The AV node & sometimes the SA node are not functioning normally! D. The axis of T-waves is in the opposite direction of the QRS complexes E. Rate = 20 – 40 bpm
2. Accelerated Idioventricular Rhythm (AIVR) A. Often develops following anacute MI! B. Occurs in short bursts & lasts < 20 sec C. Rate = 40 – 120 bpm
3. VentricularTachycardia (VT) • Once again, you see broad& bizarreQRS complexes (> 0.12 sec) B. Often with an abrupt onset C. Rate 120 – 140 bpm D. Can be monomorphicorpolymorphic(Torsades) • Look for ventricular capture & fusion beats – Capture beat: a normal atrial beat “breaks through” BEFORE the ventricular beat has occurred – Fusion beat: the atrial beat “breaks through” DURING the ventricular beat
4. VentricularFibrillation (VF) • Chaotic depolarization of the ventricles • Loss of organized QRS complexes • Complete loss of the cardiac contractile function • Circulatory arrest comes about within seconds • The most common cause of sudden cardiac death