Download
1 / 16
160 likes | 188 Views
This guide provides detailed information on diagnosing developmental disorders and mental retardation, emphasizing the importance of diagnosis in guiding treatment and establishing health maintenance plans. Key factors considered include dysmorphic signs, karyotyping, and specific diagnostic tests such as imaging studies and laboratory investigations. The epidemiological breakdown of causative factors and rationale for evaluation methods are outlined, helping healthcare professionals navigate the diagnostic process effectively. The guide concludes by stressing the significance of physical examinations and new diagnostic tools in improving diagnostic accuracy and patient outcomes.

E N D
Diagnosis • Very important • Helps to decide the treatment • Starting adequate management/treatment • Establishing the health maintenance plan • Helps to establish recurrence risk • Predicting prognosis
DEVELOPMENTAL DISORDER/MENTAL RETARDATION DYSMORPHIC OTHER NON NON NEURO SIGNS DYSMORPHIC Diagnosed unknown Karyotype Diagnosis Cherry red spot Hepatomegaly Diagnosed
DEVELOPMENTAL DISORDER/MENTAL RETARDATION DYSMORPHIC OTHER NON NON NEURO SIGNS DYSMORPHIC • Microcephalic Normocephaic • Macrocephalic • Neuro signs + Neuro signs N • CT/MRI Metabolic work up Non Specific MR • Diagnose Diagnose Fragile X syndrome
EPIDEMIOLOGY • MCA/MR syndrome 26% • (Chromosome and others) • Metabolic disorders 6% • CNS Developmental defects 16% • CP/Seizure/Hypotoni group 34% • Environmentally-Caused 13% • PureMR±Autism 5% Wisconsin study 1978
Chromosomal (including fragile X) 30% • MCA syndrome 4-5% • Metabolic disorders 3-5% • CNS Developmental defects 10-15% • Aquired causes/ injuries 15-20% • Unknown cause 25-38% • McLaren & Bryson 1987
summary 5 major causes of DD/MR • MCA syndrome • CNS Malformation • Metabolic disorder • Aquired conditions • “Pure/Non specific” MR
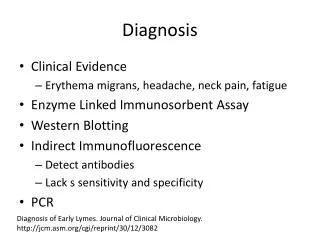
RATIONALE EVALUATION OF DD/MR Clinical Evaluation • 3 generation pedigree • Pre, peri, post natal history • Physical examination (Minor anomaly) • Neurological evaluation • Assessment of behavioral phenotype
Laboratory testing • CBC • Blood sugar • Serum calcium • Serum inorganic phosphorus • Creatinine in plasma & urine (Increased level on creatinine found in urine and plasma in X linked creatinine-transporter gene (SLC6A8) defect – mild MR, severe speech delay, hypotonia) • Metabolic testing – as indicated by clinical examination • Urine ferric chloride test • Urine DPNH test • Amino acid profile in urine / plasma
Laboratory testing • SPECT HMPAO/ ECD • Karyotyping • Fish analysis • Fibroblast karyotype • Fragile X in both male and female • Neuroimaging • Fundus examination
Laboratory testing • Arginine:Glycine amidinotransferase deficiency: • (Mild MR. Severe speech delay, with normal examination/OFC and blood creatinine levels. MRS disclosed the total absence of creatinine/phosphocreatinine peak in multiple brain areas Creatinine monohydrate oral administration restored brain creatinine levels along with improvement of the patient disability
X linked Mental retardation • 5 – 14% of MR • 130 X – Linked syndromes • MRX – 75 gene loci • Fragile X ¼ - 6,000 males • Am J Med Genet 2000, 97 (3):1
Good indicators for subtelomeric defects • Family history of MR • Prenatal onset of growth retardation • Post natal poor growth/over growth • 2 or more facial dysmorphic features • 1 or more non facial dysmorphic features and/or congenital abnormalities
Differential diagosis DD/MR Physical, neurological examination Normal finding abnormal finding Do Karyotyping/DNA fra(X) 47,xxy,fra (x) Normal results Idiopathic MR
DD/MRPhysical, Neurological examinationAbnormal finding with No major, minor anomaly
DD/MRPhysical, Neurological examinationAbnormal finding with major, minor anomaly i.e MCA/MR Subtelomeric Chromosome Diagnosis Normal results Idiopathic MCA/MR
RATIONALE EVALUATION OF DD/MR CONCLUSIONS • Through physical examination + awareness of the existence of definite patterns of malformations Newer diagnostic techniques Diagnosis