Nursing Homes as Data Collection Sites
60 likes | 228 Views
Nursing homes are complex systems with a unique culture. Nursing Homes as Data Collection Sites. Philip D. Sloane, MD, MPH University of North Carolina at Chapel Hill ABT team : Rosanna Bertrand, PhD; Lauren Olsho ; Louise Hadden ; Alrick Edwards.

Nursing Homes as Data Collection Sites
E N D
Presentation Transcript
Nursing homes are complex systems with a unique culture Nursing Homes as Data Collection Sites Philip D. Sloane, MD, MPH University of North Carolina at Chapel Hill ABT team: Rosanna Bertrand, PhD; Lauren Olsho; Louise Hadden; AlrickEdwards. UNC team: Sheryl Zimmerman, PhD; Anna Beeber, PhD, GNP, RN; Christine Kistler, MD, MASc; C. Madeline Mitchell, MURP Funding provided by AHRQ contract # HHSA 290200600001I.
Prior Research Experience ABT Team Nursing home research: • Over 20 years of NH QI research • Over 30 federally-funded intervention/evaluation studies Infection research: • Antibiogram use in NHs • Multiple US and international HIV studies UNC Team (CS-LTC) Nursing home research: • Over 25 funded NH studies over 20+ years involving primary data collection • 7 NH intervention trials Infection research: • 2 NH infection studies
Goals and Study Design • GOALS: • • Implement & evaluate a multicomponent QI program on optimizing antibiotic prescribing • • Assess the validity of the Loeb Minimum Criteria • DESIGN: • • LTC provider group / 2 geographically separate regions • • One region assigned to intervention (6 NHs) • Other assigned to comparison (6 NHs) • • 9 months chart abstraction (3m baseline, 6m follow-up) • • QI program (months 4–9) • Provider and NH staff training (Pocket Card/Referral Form) • Brochure / meetings for residents/families • Monthly data reports / meetings with facility QI teams
Main Results Percent Change in Abx Prescribing from Baseline to Follow-Up Intervention group: 26.8% reduction Comparison group: 5.3% reduction P = 0.036
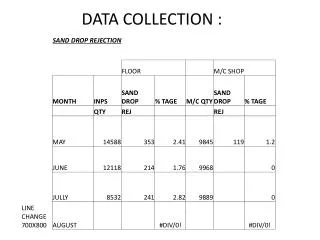
Using NH Records as Data Sources • Many NHs pre-electronic; some have EHR • Physician notes: • If electronic, access limited • If paper, quality often poor • Nursing notes: • Often quite limited; length, quality, and consistency inferior to hospital setting • Assessment data consistent, illness data not • Our attempt to introduce a standardized reporting tool for infections limited acceptance
Collecting Primary Data in NHs • No major administrative barriers encountered: NH staff cooperative • Data collection staff must be clinical (we used RNs), well trained, and supervised • Records can be massive; audit time per record was longer than we’d anticipated • Lack of systems for acute illness made standardization of data collection difficult