Download
1 / 80
830 likes | 1.14k Views
CONTENTS A 24-year-old Malay secretary with a facial rash and leg swelling Ptosis of the left eye in three patients 21-year-old Chinese teacher with progressive dysphagia Three patients with “fullness’ of the face Two patients with “scary” eyes

E N D
CONTENTS • A 24-year-old Malay secretary with a facial rash and leg swelling • Ptosis of the left eye in three patients • 21-year-old Chinese teacher with progressive dysphagia • Three patients with “fullness’ of the face • Two patients with “scary” eyes • Patients with retrosternal chest pain on exertion • 65-year-old Chinese taxi driver found unconcious • Two patients with cough and dyspnea • Two patients with cardiac murmurs • Two patients with deterioration of vision • A Malay policeman with numbness of the left side of the face • A 46-year old Indian clerk with headache and blurring of vision 6/12 • Two patients with facial swelling and oliguria • A Malay housewife with progressive lethargy • A 46-year-old Malay fisherman from Kelantan with a rash 6/12 • Two men with productive cough and decreased effort tolerance 2/12 • A 65-year-old Indian postmaster with progressive head enlargement 1 year • A 46-year-old Chinese teacher admitted with nausea and vomiting in th • background of chronic “rheumatism” • Three patients with multiple joint pain for many years • Four patients with worsening visual acuity Return to preface
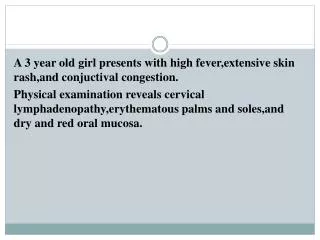
24-year-old Malay secretary with a facial rash and swelling of the legs for 3 months 1.WHAT IS THE MOST LIKELY DIAGNOSIS? Butterfly facial rash due to systemic lupus erythematosus (SLE) 2. LIST THE OTHER FEATURES USED IN THE DIAGNOSIS OF THIS DISEASE Photosensitivity Oral ulcers Arthritis Serositis Proteinuria Fits/psychosis Haemolytic anaemia/thrombocytopenia Positive LE cell/ANF/anti-dsDNA False-+ve VDRL 3. IDENTIFY THE FOLLOWING FINDINGS ASSOCIATED WITH THIS DISEASE
GANGRENE DUE TO ANTIPHOSPHOLIPID ANTIBODIES RAYNAUD’S PHENOMENON CYTOID BODIES LE CELL Click on slide for answer VASCULITIS PERICARDIAL EFFUSION 4. WHAT IS THE MOST LIKELY REASON FOR THE SWELLING OF HER LEGS? Nephrotic syndrome Click to continue
Renal involvement is very common in lupus • & can be demonstrated in renal biopsies in • almost 100% of patients by means of • electron or immunoflorescence microscopy. • Proteinuria is the most frequent abnormality • varying from trace amount to frank nephrotic • syndrome. Haematuria is frequent in severe • disease and the degree of proteinuria generally • correlates with the severity and histological • type of glomerular lesion on biopsy. The • WHO morphologicclassification of lupus • nephritis includes: • The following histologic findings in the • biopsy indicate “ACTIVITY” and unless • aggressively treated, may lead to progressive • (and sometime rapid) renal failure: • Disruption of capillary walls • Polymorphs and karyorrhexis • Hematoxyphil bodies • Crescent • Hyaline thrombi • Segmental fibrin deposition II Pure mesangial alteration I Normal glomerulus III Focal segmental glomerulonephritis IV Diffuse glomerulonephritis V Diffuse membranous glomerulonephritis VI Advanced sclerosing glomerulonephritis
2. LIST ALL THE FEATURES OF THE COMPLETE SYNDROME • Complete ptosis • Divergent strabismus (eye ‘down and out’) • Dilated pupils unreactive to direct light and to • accommodation (the consensual reaction in the • opposite eye is intact) • 1.WHAT COMMON DIAGNOSIS • HAS THESE 3 PATIENTS? Left occulomotor nerve (3rd cranial nerve) palsies 3. USING APPLIED ANATOMY, DESCRIBE HOW YOU CAN LOCALISE THE SITE OF THE LESION
Internal carotid artery 7. Supr. orbital fissure 1.The nuclear complex is situated in the midbrain. Lesion of the nucleus cause an ipsilateral 3rd nerve palsy with ipsilateral sparing and contralateral weakness of elevation. 2+3.Benedikt syndrome involves the fasciculus as it passes through the red nucleus producing ipsilateral 3rd nerve palsy and contralateral hemitremour. Weber syndrome is characterized by ipsilateral 3rd nerve palsy and contralateral hemiparesis. 6. Cavernous Poatr. communicating artery 5. Basilar III VI IV 4. Root 4+5.The basilar part of the nerve then leaves the midbrain, passes between posterior cerebral and superior cerebellar arteries, running lateral to & parallel with the poaterior commu- nicating artery. Isolated 3rd nerve palsy is usually basilar eg. aneurysms at the junction of the posterior communica- ting and internal carotid arteries and tentorial herniation of the temporal lobe resulting from extra or subdural haematoma.The pupil is fixed and dilated. 3. Ventral fascicular Weber,s) Red nuclei 2..Dorsal fascicular (Benedikt,s) 1.Nuclear Postr. cerebral artery Supr. Cerebellar artery Click to continue
6.The cavernous part runs on the lateral wall superior to the 4th nerve. In the anterior part of the cavernous sinus, it divides into superior and inferior branches before entering the orbit through the superior orbital fissure. Intracavernous 3rd nerve palsies are usually associated with 4th and 6th nerve and the 1st division of the 5th nerve; the pupils is usually spared. eg. diabetes, pituitary apoplexy, aneurysms, meningio- mas, carotid-cavernous fistula, Tolosa-Hunt syndrome (granulomatous inflammation) 7.Within the orbit, the superior division innervates the levator and superior rectus muscle. The inferior division innervates the rest plus the parasym- pathetic fibres from the Edinger-Westphal subnucleus. Fixed and dilated, unreactive to direct light and accommodation (consensual reflex in the opposite eye is normal) 5.THE PUPILLARY CHANGE IN 3rd NERVE PALSY IS IMPORTANT. EXPLAIN.
Blood vessels on pia mater supply surface of the nerve including pupillary fibres (damaged by compression) The pupillomotor parasymparasympathic fibres between the brain stem and caver- nous sinus are located superficially in the superior median part of the 3rd nerve. Blood supply of this part comes from the pial mater vessels, whereas the main trunk of the nerve is supplied by the vasa nervorum. Thus: SURGICAL lesions eg, aneurysms, trauma, & uncal herniation involves the pupil by compression whereas MEDICAL lesions eg. hypertension, diabetes usually spare the pupil because the microangiopathy associated with these medical lesions involves the vasa nervorum, causing neural infarction of the trunk of the nerve, but sparing the superficial pupillary fibres. Vasa vasorum supply part of nerve but not pupillary fibres (damaged by medical lesions) Pupillary fibres lie dorsal and peripheral Anatomy of the location of the pupillomotor fibres within the trunk of the 3rd nerve 6.THESE PATIENTS HAVE COMPLETE 3rd NERVE PALSIES. CAN YOU IDENTIFY THE CAUSE?
DIABETES L. ZOOSTER OPHTHALMICUS UNCAL HERNIATION DUE TO SUBDURAL HAEMATOMA Click on the slide for answer WEGENER’S GRANULOMATOSIS PITUITARY TUMOUR ANEURYSM POSTERIOR COMMUNICATING ARTERY
21-year-old Chinese teacher presented with progressive difficulty in swallowing for 6 months • 1.WHAT IS THE MOST LIKELY DIAGNOSIS? • 2. IDENTIFY THE SIGN IN THE PICTURE • THAT SUPPORTS YOUR DIAGNOSIS • 3.WHAT IS THE SIGNIFICANCE OF THE • SURGICAL SCAR OVER THE STERNUM? Myasthenia gravis Bilateral ptosis It is most likely that she had undergone a thymectomy recently. This neuromuscular disorder characterized by weakness and easy fatigability due to a decrease in the number of available acetylcholine receptors at the neuromuscular junctions as a result of antibody- mediated autoimmune attack. The thymus appears to be responsible for this attack, being abnormal in about 75% of patients; in about 65% the thymus is “hyperplastic”, while 10% has thymomas. 85% of patients improve after thymectomy. 4.DESCRIBE THE BEDSIDE DIAGNOSTIC TEST FOR THIS CONDITION Click for answer
BEFORE TENSILON AFTER TENSILON Click to continue Tensilon (Edrophonium hydrochloride) Test Edrophonium hydrochloride (a short acting anticholinesterase) inhibit the enzyme acetyl- cholinesterase to allow acetylcholine to interact repeatedly with the limited number of acetylcholine receptors, producing improvement in strength of myasthenic muscles. An initil dose of 2 mg is given IV. If definitive improvement is observed in the affected muscle (eg, ptosis or diplopia), the test is considered positive. Higher dose (up to 8 mg) may be required in some patients. False positive tests occur in some patients with amyotrophic lateral sclerosis and in placebo-reactors.
5.THIS 55-YEAR-OLD CARPENTER HAS MYASTHENIA GRAVIS. CAN YOU IDENTIFY THE EXTRAOCULAR MUSCLES INVOLVED? Click on picture for answer R SUPERIOR RECTUS L INFERIOR RECTUS R INFERIOR OBLIQUE L SUPERIOR OBLIQUE
1.WHAT IMPORTANT SIGN IS PRESENT IN THESE 3 PATIENTS? 2.WHAT IS THE MOST LIKELY CAUSE FOR THIS SIGN? 3.THESE FOUR OTHER SIGNS OCCURRED IN PATIENTS WITH A SIMILAR CONDITION. WHAT ARE THEY AND WHAT IS THE MECHANISM? Superior vena cava obstruction Bronchogenic carcinoma of the lungs
Click on picture for answer L Horner’s syndrome Thoracic outlet syndrome with lymphatic obstruction of the L arm Dilated superficial chest and abdominal wall veins. Blood flows downward and eventually reenters the inferior vena cava via the femoral vein. Wasting of hypothenar muscles due to T1 involvement in thoracic outlet syndrome Click to continue
4.IDENTIFY THE 2 IMPORTANT FEATURES OF HORNER’S SYNDROME IN THIS PATIENT. WHAT IS THE MECHANISM? Click on picture for answer • Partial L ptosis : interruption of sympathetic • innervation of the smooth muscles of the eyelid • Constricted L pupil which reacts normally to light • (unbalanced parasympathetic action) The 3-neurone pathway projects from the hypothalamus to the intermediolateral column of the cervical spinal cord, then to the superior cervical ganglion and finally to the pupil, the levator palpebrae and the sweat glands of the face. A lesion at any site along the pathway can produce Horner’s syndrome. 7.LIST THE IMPORTANT CAUSES OF HORNER’S SYNDROME 5.WHAT ARE THE OTHER FEATURES OF THE SYNDROME? • Decrease sweating of the L face (anhydrosis) • Enophthalmos (retraction of the eyeball) 6.DESCRIBE THE OCULOSYMPATHETIC PATHWAY INVOLVED IN THE SYNDROME
CAUSES OF HORNER’S SYNDROME Central Brainstem disease (tumour, vascular, demyelination) Syringomyelia Lateral medullary (Wallenburg) syndrome Spinal cord tumour Preganglionic Pancoast tumour Carotid & aortic aneurysms/dissections Lesions in the neck (malignant nodes, trauma, surgery) Postganglionic Cluster headaches (migraine neuralgia) Nasopharyngeal CA Otitis media Carvenous sinus mass Internal carotid artery disease 8.THIS 60-YEAR-OLD TAXI-DRIVER HAS CARCINOMA OF THE LUNG. WHAT COMPLICATION HAS OCCURRED?
Endocrine changes Hypercalcemia due to PTH-like substances Hyponatremia due to ADH Ectopic ACTH syndrome Carcinoid syndrome Gynaecomastia due to gonadotrophins Hypoglycaemia due to insulin-like peptide Neurologic manifestations Eaton-Lambert syndrome Peripheral neurppathy Subacute cerebellar degeneration Polymyositis Cortical degeneration Haematological features Migrating venous thrombophlebitis Disseminated coagulation Anaemia Skin Acanthosis nigricans Renal Nephrotic syndrome due to membranous glomerulonephropathy DERMATOMYOSITIS (heliotrope rash with periorbital edema) Click for answer 8.LIST THE NON-METASTATIC EXTRAPULMONARY MANIFESTATIONS OF CARCINOMA OF THE LUNGS
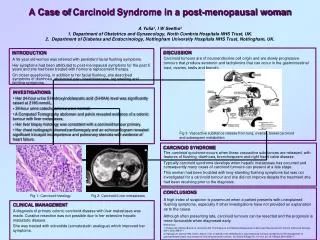
1.WHAT IS YOUR DIAGNOSIS? 2.IN CONTRAST TO OTHER CAUSES OF THYROTOXICOSIS, WHAT ARE THE DISTINGUISHING FEATURES OF THIS DISEASE? 3.LIST THE FEATURES OF OPHTHALMOPATHY Graves’ disease Diffuse goiter Ophthalmopathy Localized dermopathy Lymphoid hyperplasia Thyroid acropachy
FEATURES OF OPHTHALMOPATHY IN GRAVES’ DISEASE • Grittiness and discomfort in the eye • Retrobulbar pressure or pain • Eyelid retraction in the primary gaze (Dalrymple sign) • Eyelid lag (Von Graefe sign) • Kocher sign is a staring and frightened appearance • Periorbital edema, chemosis and scleral injection • Extraocular muscle dysfunction • Exposure keratitis • Optic neuropathy • Exophthalmos Click to continue
4.THESE PATIENTS HAVE THYROTOXICOSIS. WHAT DO THEY SHOW? PROXIMAL MYOPATHY PALMAR ERYTHEMA Click on picture for answer SEVERE WASTING THYROID ACROPACHY (pseudo-clubbing) PRETIBIA MYXOEDEMA Characterized by lymphocytic infiltration of the dermis, accumulation of glycosaminoglycans and edema Click here to continue
4.THIS 45-YEAR-OLD CARPENTER HAS GRAVE’S DISEASE. WHAT IS THE RELATIONSHIP BETWEEN THE 2 PICTURES? 5.LIST THE OTHER CONDITIONS THAT MAY BE ASSOCIATED WITH GRAVES’ DISEASE Bilateral ptosis due to association of myasthenia gravis & Graves’ disease Type 1 diabetes mellitus Addison’s disease Vitiligo Pernicious anaemia Alopecia areata Celiac disease
1.WHAT ARE THESE TWO PATIENTS SUFFERING FROM? 2.WHAT OTHER SIGNS WILL YOU LOOK FOR TO SUPPORT YOUR DIAGNOSIS? Hyperlipidaemia (xanthelesma around the eyes)
ARCUS SENILIS (corneal arcus) XANTHOMATAS 3.HOW DO YOU CLASSIFY THE PRIMARY HYPERLIPIDAEMIA?
PRIMARY HYPERLIPIDAEMIA (WHO modification of Fredrickson classification) Type Pl. cholesterol Pl. triglyceride Defect Inheritance/ Atherosclerosis Prevalence risk l normal (chylo) Lipoprotein lipase recessive No deficiency (rare) lla LDL normal LDL receptor defect dominant Yes (common) llb LDL VLDL LDL receptor defect dominant Yes (common) Lll IDL Apo E abnormality - Yes (rare) lV normal or slight VLDL Overproduction of dominant No VLDL (common) V normal or slight chylo & Lipoprotein lipase recessive No VLDL deficiency (rare) Click to continue
4.HOW CAN THESE 2 PICTURES HELP YOU DIFFERENTIATE BETWEEN HYPERCHOLESTEROLAEMIA & HYPERTRIGLYCERIDAEMIA? This 60-year-old house had coronary artery by-pass surgery recently as evidenced by the sternotomy surgical scar. Lipid deposition in soft tissue (eg. xanthelesma [as in this patient], tendon & palmar xanthomata, corneal arcus) always indicate hypercholesterolaemia. Hypercholestronaemia is a major risk factor for coronary artery and peripheral vascular diseases. This patient has severe hypertriglyceridaemia as evidenced by the creamy supernatant simply by storing plasma for 18 hours at 40C. 5.WHAT OTHER FEATURES ARE ASSOCIATED WITH HYPERTRIGYCERIDAEMIA?
ACUTE PANCREATITIS ERUPTIVE XANTHOMATA LIPAEMIA RETINALIS 6.WHAT ARE THE SECONDARY CAUSES OF HYPERLIPIDAEMIA?
SECONDARY HYPERLIPIDAEMIA Cholesterol Complications Disorder VLDL LDL HDL Triglycerides Diabetes or CHD Obesity CHD Hypothyroidism - - CHD Nephrotic syndrome - CHD Cholestasis(.eg primary biliary cirrhosis) - - - CHD Alcohol abuse - or pancreatitis 7.WHAT WILL BE YOUR CHOICE OF DRUGS IN HYPERLIPIDAEMIA?
1.THIS 65-YEAR- OLD CHINESE TAXI DRIVER WAS FOUND UNCONCIOUS IN BED BY THE FAMILY. WHAT IS THE MOST LIKELY REASON? 2.WHAT IS THE MOST LIKELY CAUSE OF THE CONDITION IN THIS PATIENT 3.IDENTIFY 4 SIGNS IN THE PICTURES THAT WILL SUPPORT YOUR DIAGNOSIS Hepathic encephalopathy Cirrhosis • Jaundice • Gynaecomastia • Spider naevi on the abdomen • Portal hypertension (dilated abdominal veins • and ascites) Click to continue
4.THESE CONDITIONS ARE IMPORTANT CAUSES OF FULMINANT LIVER FAILURE. WHAT ARE THEY? ACUTE VIRAL HEPATITIS ALCOHOLIC HEPATITIS Peroxidase positive particles Mallory hyaline bodies Click on picture for answer DRUG-INDUCED HEPATITIS eg. aspirin, INH, rifampicin PARACETAMOL POISONING LEPTOSPIROSIS Click to continue
4.WHAT IS THIS SIGN IN A PATIENT WITH HEPATIC ENCEPHALOPATHY? WHAT IS THE MECHANISM? 5. IN A PATIENT WITH LIVER FAILURE, STANDING CLOSE TO THE PATIENT MAY REVEAL THE DIAGNOSIS. WHY? 6.WHAT ARE THE CLINICAL STAGES OF HEPATIC ENCEPHALOPATHY? Hepatic flap (asterixis) : Jerky, irregular flexion- extension movement at the wrist and metacarpo- phalangeal joints, often accompanied by lateral movements of the fingers. It is possibly due to the interference with the inflow of joint position sense information to the recticular formation in the brain- stem resulting in rhythmical lapses of postural muscle tone. Flap is usually bilateral, absent at rest, and is brought on by sustained posture. Fetor hepaticus is a unique musty odor of the breath or urine due to the presence of mercaptans
CLINICAL STAGES OF HEPATIC ENCEPHALOPATHY Stage Mental Status Asterixis EEG* I Euphoria or depression, mild confusion, + / - Normal slurred speech, disordered sleep II Lethargy, moderate confusion + Abnormal III Marked confusion, incoherent speech, + Abnormal sleepy but arousable IV Coma, initially responsive to painful - Abnormal stimuli, later unresponsive *EEG : Characteristic symmetrical, high voltage, slow waves (2-5 per second) pattern
1.WHAT IS YOUR DIAGNOSIS? 2.IDENTIFY TWO IMPORTANT SIGNS TO SUPPORT YOUR DIAGNOSIS. Chronic obstructive airway disease (COAD) Click to continue • Central cyanosis • Barrel-shaped chest
3.THESE TWO PATIENTS SUFFER FROM COAD. WHAT ARE THE DIFFERENCES? Predominant Predominant emphysema bronchitis Age at time of onset 60± 50± Dyspnea severe mild Cough after dtspnea starts before dyspnea starts Sputum scanty, mucoid copious, purulent Bronchial infections less common Respiratory failure often terminal repeated episodes CXRs hyperinflated ± increased bronchovascular bullous changes, markings at base, large small heart heart Chronic PaCO2 mmHg 35-40 50-60 Chronic PaO2 mmHg 65-75 45-60 Haematocrit (%) 35-45 50-55 Pulmonary hypertension none to mild moderate-severe Cor pulmonale rare common Elastic recoil severely decreased normal Resistance normal, slight increase high Diffusing capacity decreased normal to slight decrease BRONCHITIS EMPHYSEMA Click to continue
4.THESE FEATURES IN COAD DIFFERENTIATES BETWEEN TYPE 1 AND TYPE 2 RESPIRATORY FAILURE. WHAT ARE THEY? WARM, DRY HAND WITH DILATED SUPERFICIAL VEINS PAPILLOEDEMA DROWSINESS Click on picture for answer FLAPPING TREMOUR Click to continue
5.WHAT IS THE DANGER WHEN YOU ADMINISTER O2 TO THESE PATIENTS WITH COAD? (click for answer) REGULATION OF RESPIRATION HYPOXIC DRIVE Patients with long-standing COAD and Type 2 respiratory failure depends on their hypoxic respiratory drive to ventilation. Removal of this drive by administering O2 will lead to further hypoventilation, large increase in PaCO2, intracerebral vascular dilatation, raised intracranial pressure, papilloedema, stupor, and coma. Patients most at risk to for O2-induced CO2 retention are those presenting with PaO2 below 50 mmHg and pH <7.26.
6.WHAT IS THIS MEASUREMENT? normal obstructive restrictive 7.WHAT DOES THIS GADGET MEASURE? Peak expiratory flow rate (PEFR). Obstructive lung disease eg. COAD and asthma will give a low measurement This is a forced expiratory spirogram. Starting with a full inspiration the volume expired during a forced expiration (forced vital capacity, FVC) is reduced in both obstructive and restrictive pulmonary disease (eg. lung fibrosis). However, the volume expired in 1 second (FEV1) is disproportionately reduced in patients with airway obstruction (eg. chronic bronchitis and much less so in emphysema) Click to continue
7.THESE PATHOGENS ARE COMMONLY INVOLVED IN ACUTE EXACERBATION OF COAD. NAME THEM? Click on the picture for answer Streptococcus pneumonia Haemophilus influenzae Mycoplasma pneumoniae
35-year-old Malay housewife with progressive dyspnea on exertion 1/12 28-year-old unemployed Malay man was found unconscious by the roadside 1.WHAT IS THE ABNORMALITY IN THE EYE? 2.WHAT IS THE SIGNIFACANCE OF THIS FINDING? 3.WHAT OTHER FINDINGS WILL YOU LOOK FOR IN BOTH PATIENTS? Subconjunctival haemorrhage Infective endocarditis Click here for answer
SPLINCTER HAEMORRHAGE : subungual linear “vasculitic” lesions OSLER’S NODES: red, raised tender nodules on the pulp of the fingers (or toes), or on the thenar or hypothenar eminences ROTH’S SPOT : intraretinal haemorrhages with white certres representing fibrin thrombus occluding a rupture blood vessel CLUBBING JANEWAY’S LESION: Non-tender, erythematous maculopapular lesions, containing bacteria, which occur very rarely on the palms and pulps of the fingers Click to continue
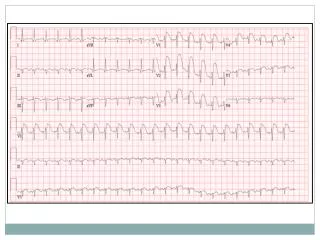
4.THIS IS THE CXR, PHONOGRAM, AND ECG OF THE 35-YEAR-OLD MALAY HOUSEWIFE. WHAT IS THE MOST LIKELY LESION IN HER HEART? Click for answer Atrial septal defect (ostium secundum type). The physical signs are the result of RVH and increased flow through the right causing pulmonary and tricuspid flow murmur and fixed wide splitting of the 2nd heart sound. ECG shows R axis deviation and RBBB. In contrast, ostium primun type defect show L axis deviation ECG S1 A2 P2 Phono Click to continue
5.THIS IS THE LEFT ARM, CT BRAIN, AND ECHOCARDIOGRAM OF THE 28-YEAR-OLD MALAY MAN. WHAT IS YOUR DIAGNOSIS? 6.WHICH IS THE MOST LIKELY ORGANISM CAUSING IT? Intrvenous drug user with infective endocarditis and brain abscess due to embolism Staphylococcus aureus Click to continue
7.URINANALYSIS OF THIS PATIENT REVEALED THE PRESENCE OF HAEMATURIA AND PROTEINURIA. WHAT IS THIS? This is a RBC cast in a urinary sediment. They are always abnormal and indicate the presence of primary glomerular disease. 8.IN VIEW OF THE URINARY ABNORMALITIES, A RENAL BIOPSY WAS PERFORMED. WHAT IS THE PATHOLOGY? The biopsy show focal segmental glomerulonephritis with thrombosis (), necrosis,cellular proliferation and early segmental crescent most probably provoked by immune complex deposition. IF microscopy commonly demonstrates granular deposits of IgG and C3 and sometimes other immune globulins. EM shows electron dense mesangial, subendothelial, and subepithelial deposits. Fibrin is seen in the necrotic areas.
1.IDENTIFY 3 ABNORMALITIES IN THESE PICTURES 2.WHAT IS THE CAUSE? 3.WHAT IS THE PATHOGENESIS? • Microaneurysms • Exudates • Neovascularization Diabetes mellitus Diabetic retinopathy has features of both microvascular occlusion and leakage. The microvascular occlusion is due to a combination of capillary basement membrane thickening, endothelial cell damage and proliferation, deformation of RBCs, and increased platelet stickiness and aggregation.. Occlusion leads to non-perfusion ischaemia, retinal hypoxia.and neovascularization caused by ‘vasoformative substance” (growth factors) elaborated by hypoxic renal tissue in an attempt to revascularize hypoxic areas of the retina. The retinal capillaries consist of endothelial cells and pericytes (mural cells). The tight junctions of the endothelial cells constitute the inner blood-retinal barrier. The pericytes are wrapped around the capillaries and are responsible for the structural integrity of the vessel wall. In diabetes, the numbers of pericytes are reduced resulting in distension of capillary walls and breakdown of the blood-retinal barrier, leading to microvascular leakage of plasma constituents into the retina. Microaneurysms are saccular pouches due to local capillary distension. The consequences of increased vascular permeability are intraretinal haemorrhage and oedema which may be diffuse or localized. Chronic localized retinal oedema leads to the deposition of hard exudates (composed of lipoprotein and lipid-filled macrophages) at the junction of normaal and oedematous retina. 4.WHAT IS THE CLINICAL IMPORTANCE OF THE ABOVE RETINAL CHANGES?
. CORONARY ARTERY DISEASE KIMMELSTIEL-WILSON LESION DIGITAL GANGRENE Click on picture for answer DIABETIC DERMOPATHY CEREBRAL VASCULAR DISEASE PERIPHERAL NEUROPATHY Click to continue
6.WHAT COMPLICATION HAS OCCURRED IN THESE DIABETIC RETINOPATHIES? Branch retinal vein thrombosis Subhyoid haemorrhage Vitreous haemorrhage Burnt-out stage of diabetic retinpathy
This is a 52-year old policeman who presented with numbness on the left side of the face 1.IDENTIFY THREE ABNORMALITIES IN THE PICTURES 2.WHAT IS THE DIAGNOSIS? Decreased left nasolabial fold Weakness of the left facial muscles around the angle of the mouth Weakness of the left occipital frontalis muscle on attempted elevation of the brow Left facial nerve palsy (lower motor neurone type) Click to continue
3.THE FOUR PATIENTS HAVE 7th CRANIAL NERVE PALSIES. WHAT IS THE CAUSE? 1.Abscence corneal reflex and/or involvement of the 8th CN suggest that the lesion is located at the cerebellopontine area or internal auditory meatus 2.Complaint of hyper- acusis on the ipsilateral side suggest that the lesion is located in the region of the middle-ear (paralysis of the stapedius bone), or loss of taste to the anterior 2/3 of the tongue (involvement of the chorda tympani nerve travelling with the lingual nerve). This type of lesions may complicate otitis media. PAROTID TUMOUR or SARCOIDOSIS 4.WHAT OTHER FEATURES MAY HELP IN THE LOCALIZATION OF THE LESION? BELL’S PALSY (Bell’s phenomenon on the left. Lesion is located at the level of the petrous temporal bone) Click on picture for answer PONTINE LESION (suggested by associated 6thCN palsy plus contralateral hemiplegia) RAMSAY-HUNT SYNDROME (associated ear/palatal vesicles of herpes zooster infection of the geniculate ganglion) Click to continue
7. 5.THIS 16-YEAR-OLD MALAY STUDENT HAS BILATERAL 7th CRANIAL NERVE PALSIES. WHAT ARE THE POSSIBLE CAUSES? • Guillain-Barre syndrome • Sarcoidosis • Bilateral parotid disease • Lyme disease • Mononeuritis multiplex (eg diabetes, PAN) Click to continue
6.THIS 60-YEAR-OLD CHINESE HOUSEWIFE HAS R FACIAL WEAKNESS. WHERE IS THE LESION 7.IN CONTRST TO 7th CRANIAL NERVE PALSY (LMN TYPE), WHY IS THERE SPARING OF THE UPPER HALF OF THE FACE IN INTERNAL CAPSULE LESIONS? X INTERNAL CAPSULE A lesion here will cause R hemiplegia (due to damage of the cortico- spinal tract fibers) and mild R facial weakness with sparing of the brows (upper ½ of the face) due to the bicortical innervation of the occipital frontalis muscles upper ½ of the face The sparing of the R occipital frontalis muscles places the lesion above the pons and the most likely site is in the left internal capsule (7thcranial nerve palsy,UMN type). This patient will have associated R hemiplegia.
This 46-year-old Indian clerk presented with headache and blurring of vision in the left eye 6/12 1.WHAT IS YOUR DIAGNOSIS? Acromegaly 2.IDENTIFY 4 FEATURES IN THE PICTURES TO SUPPORT YOUR DIAGNOSIS 3.WHAT IS THE MOST LIKELY REASON FOR THE BLURRING OF VISION HOW CAN YOU CONFIRM IT ON PHYSICAL EXAMINATION? WHAT IS THE EXPECTED FINDING? • Prominent supraorbital ridges • Enlargement of nose • Thickening of lips • Smooth, shinny skin due to • increase sebum production The blurring of vision is due to compression of the optic chiasma by a pituitary tumour. This can be confirmed by charting the visual field (using confrontation technique) during physical examination. The expected typical finding is bitemporal hemianopia however in the early stages of the tumour, this field defect may not be complete. In advance cases the patient can develop optic atrophy. Click to continue