Download
1 / 43
430 likes | 517 Views
Dr. Ramon Figueroa presents Belize's National Health Insurance model with strategic objectives, pilot project, results, and future plans for health reform and system enhancement in the English-speaking Caribbean region.

E N D
Meeting of Directors of Social Security Organizations in the English-speaking Caribbean Presentation by Dr. Ramon Figueroa, Social Security Board Belize
OUTLINE OF PRESENTATION • INTRODUCTION- Case for NHI • Conceptual Design: • Vision of the New Health System • Strategic objectives • Paradigm shift • Pilot project • Package • Results
OUTLINE OF PRESENTATION • Post-Pilot: • Extensions • Changes • Results • Where we are now • Financing • Schedule of roll-out • Model • Lessons learned
MEXICO G U A T E M A L A
INTRODUCTION • Population: 282,600 (2004 mid-year estimate) • Rural (141,600); Urban (141,000) • Land area: 23,000 squ. Km (8867 sq. Mls) • Administratively divided into six districts. • Multiethnic society (garifuna, maya, creole, mestizo, chinese, East Indian, Mennonite) • Primary Income earners: Tourism, Agriculture, shrimp farming. • GDP Per capita 3,753 US (2004). • Unemployment rate at 11.6 % (2004) • Poverty rate at 33.5 % (LSMS 02) • Health Expenditure (4.7 % of GDP); 52 % public and 48 % private expenditures; 176 US per capita (1997)
INTRODUCTION (CONT.) • Challenges*: • Ineffective and inefficient public system; • Under-funded health system; • Poor accountability, discipline, attendance and “customer service”; • Few meaningful incentives within public sector; • Over-centralized command and control in MOH with too many vertical programs; • Haphazard and limited growth of private sector; • Misallocation/insufficiency of resources in public sector. *Belize Ministry of Health and Sports Health Policy Reform Project, Final Report, Prepared by CCC, August 7, 1998
VISION “We envision a national health care system which is based on equity, affordability, accessibility, quality and sustainability in effective partnership with all levels ( sectors ) of government and the rest of society, in order to develop and maintain an environment conducive to good health.”
HEALTH REFORM “Health Sector Reform is a process aimed at introducing substantive changes in the different structures and functions of the sector, with a view to increasing the equity of its benefits, the efficiency in its management, and the effectiveness of its actions; and through this to achieve the satisfaction of the health needs of the population. It is an intense phase of transformation of the health systems based on situations that justify and make it viable.”
STRATEGIC OBJECTIVES • Develop the function of MOH to become a strong regulatory and policymaking entity. • Decentralization of responsibility and accountability. • Development of internal market mechanisms. • High degree of flexibility. • Clear separation of financing and delivery. • Gradual introduction of competition in quality and efficiency. • Ensure greater accountability to patients. • Seek value for money.
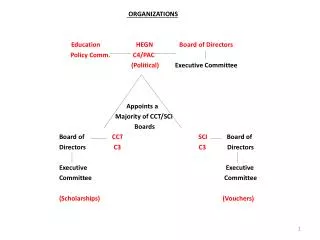
PARADIGM SHIFT PROVIDER REGULATOR SEPARATION OF FUNCTIONS SEPARATION OF FUNCTIONS PURCHASER USER
PILOT PROJECT • Population of 36,853 in economically deprived area of city. • Officially launched by PM on 9th Aug, 2001 • Project was officially “ended” Feb 12th, 2002: Evaluation conducted • Parameters: 1 physician team per 4,000 population • Group practice model • Tendering process followed. • Evaluation of facilities to ensure basic standards met. • Contractual agreement established • Contractor Generals office involved. • Included: • Primary care providers- 4 (3 private and 1 public)- • Pharmacies-5 private • Laboratories-3 private • imaging services-3 private • Hospitals-3 (1 public and 2 private) • Ophthalmology-3 private –
Services included in the PHC Package... Based on needs for a population of 4,000
Services included in the PHC Package (cont…)
Specialist Services included in the Hospital Package... • Obstetrics • Gynecology • Internal Medicine • Pediatrics • Surgery • Orthopedics • Ophthalmology • Dermatology • Outpatient Surgery • Urology • Neurology Including all specialist services currently offered in Belize • Contracting limited to budget cap of NHI • Contracting at pre-established Price • Contracting only with accredited specialists • Control of specialists consultations by hospital
ANALYSIS OF RESULTS: Equity and Access Table 9: NHI improvement in physical access of health services Supporting Facts Pre-Pilot Post-Pilot B. Respondents who are within 30 minutes walking distance to clinic 37% 50% C. Respondents who wait < 30 minutes once at clinic 38% 44% Source: University of Belize Pre-pilot survey data and SPEAR Post-Pilot survey data
Equity and access (cont.) • qIn terms of access to specific services : • o1. 55% of population of women 40-69 years of age were screened for breast cancer. • o2. 51% of target population of men > 50 years of age were screened for prostate cancer. • o3. 31%of target population of women 30-69 years of age were screened for cervical cancer. • At the Primary level, • the ratio of GP/1000 population increased from 0.05 pre-pilot to 0.32 during pilot thus increasing accessibility of population to a General Practitioner. • The ratio of Nurse/1000 population increased from 0.11 to 0.6 per 1000 population. • Total clinic hours open to the public increased by 3.7 times/day (normal week days) but was only open for 4 hours on weekend. • q
Equity and access (cont.) Table 10: Improved access to the most appropriate level of care Supporting Facts Pre-Pilot Post-Pilot B. Respondents who need to see and have seen specialist 36 % D. Respondents who cannot afford medication prescribed 24 % 2 % E. Respondents receiving medication with no cost at point of service 34 % 100 % F. Respondents who receive healthcare services with no cost at pt of service 60 % 100 % G. Respondents who have been prescribed lab tests 37 % Percent that received it with no cost at point of service 67 % 100 % H. Respondents who have been prescribed imaging tests 41 % 35 % Percent that received it with no cost at point of service 40 % 100 % Source: University of Belize Pre-pilot survey data, and SPEAR Post-Pilot survey data A. Respondents attended by GP 40 % 90 % 98 % 55 %
Efficiency and Productivity • qThe volume of care delivered to the population was significant: • 1. 21,588 total consultations made by four Primary Care Providers[1]. • o 2. 495 total hospitalizations from one public and one private institution. • o 3. 13,901 total prescriptions given out. • o 4. 4,213 total imaging referrals made. • o 5. 6,091 total laboratory referrals made. • o 6. 688 total eyeglasses given to children between ages of 7 to 19. • o 7. 129 total cataract surgeries performed. • o 8. A total of 2,220 specialist visits were made. • o9. 1,100 people from outside the pilot project area received medical care • qThe primary care clinics improved the efficiency of the system as evidenced by a reduction in population seeking specialist care without a referral. • a. Prior to pilot implementation there were approximately 341 outpatient consultations per 1000 population per annum without a referral in Belize South Side, versus 76 per 1000 population per annum. • qb. Ninety percent of all respondents used the GP as means of entry into the system, versus only 40% prior to the pilot project. • q
Effectiveness and Quality • q Five major protocols were developed during the Pilot Project: Asthma, Diabetes, Hypertension, Congestive Heart Failure, and Myocardial Infarction. • qAll physicians and nurses participating within the provision of services in the Pilot were trained in the use of the protocols. • qMedical Audits were conducted to evaluate the application of the Asthma, Diabetes and Hypertension protocols at the primary level.
Effectiveness and Quality Table 18: Explanation of tests and treatments Supporting Facts Pre-Pilot Post-Pilot A. Respondents that wait < 30 minutes for lab tests 48 % 58 % Respondents that have test results explained to them 89 % 100 % B. Respondents that wait < 30 minutes for imaging tests 58 % 69 % Respondents that have test results explained to them 90 % 99 % C. Respondents that receive full treatment explanation from doctor 58 % 89 % Source: NHI data and University of Belize Pre-pilot survey data, and SPEAR Post-Pilot survey data
Effectiveness and Quality Table 19: Perception of healthcare Supporting Facts Pre-Pilot Post-Pilot A. Respondents that believe they are receiving the best healthcare possible 20 % 61 % B. Respondents that are always treated with courtesy and respect 59 % 90 % C. Respondents that spend more than 15 minutes with GP 37 % 75 % Respondents that feel that doctor always explains treatment fully 58 % 88 % Source: NHI data and University of Belize Pre-pilot survey data, and SPEAR Post-Pilot survey data
Effectiveness and Quality Table 21: Percentage of Patient Satisfaction by PCP PCP Qualification BFLA 86 % IHC 85 % BMA 81 % MRHC 75 % Source: NHI/MOH survey data and Sanigest International Analysis
Table 22:Patient Satisfaction Survey Results by Hospital Effectiveness and Quality Hospital Percentage Satisfaction Private 89 % Public 69 % Source: NHI/MOH survey data and Sanigest International Analysis
Effectiveness and Quality Table 24: Protocol implementation Provider Asthma Hypertension Diabetes BMA 75 % 75 % 57 % BFLA 63 % 75 % 57 % IHC 75 % 75 % 57 % MRHC 50 % 75 % 57 % Source: NHI protocol evaluation data and Sanigest International Analysis
SOCIAL PARTICIPATION Table 14: PCP members and transfers PCP Members per PCP Members transferred to another PCP as a percentage of total members Members transferred to the PCP as a percentage of total members Difference BFLA 3442 8 % 10 % 2 % BMA 4650 3 % 12 % 9 % IHC 8743 8 % 3 % -5 % MRHC 4447 9 % 7 % -2 % Total 21282 7 % 7 % 0 % Source: NHI data system
Source: Ministry of Health data; NHI data; Sanigest analysis
The NHI South Side Project-Post-Pilot • Extensions (5 total from Feb 12th, 2002 to May, 2003)…addendums-Adjustment of Hospital package, introduction of co-payments (support services) • Financial limitations (SSB financing scheme) • New Contracts June 2003-March 2004 • PMPM changed from $7.03 to $6.30 (70/30) • Changes in package of services: co-payments, limited hospital services (deliveries). • Extended April to Dec 2004; • Extended Jan05 to March, 2006)
CLINICAL RECORD AUDIT RESULTS (AUGUST 2004) • MRHC ………….78 % • BFLA…………….63 % • IHC………………61 % • BMA……………..45 %
FINANCIAL PERFORMANCE (2004) • Expected expenditure to date should be 100 %(April to Dec 04) • Total NHI Expenditure……………81.4 % • PCP expenditure………..96 % • Lab expenditure…………76.5 % • Imaging expenditure……47.6 % • Pharmacy expenditure….71 % • Ophthalmology…………..25.7 % • Hospital services…………88.9 %
SUMMARY • Contracts extended up till March of 2006 for the South Side of Belize City. • PMPM adjustment..($4.41 + $1.89 presently) • Expenditures kept under control using Monthly Incentive Scheme (performance benchmarks) • Cabinet decision to roll to the South of country, based on the public sectorstrengthening. • Long term financing source still a question. • Medium term financing by SSB, MOH, Gob.
Draft Schedule for Roll-Out • 2005-2006……South Side Belize+ Toledo+ Stann Creek. • 2006-2007……Add North of Belize District + Corozal + Orange Walk • 2007-2008……Add Cayo District.
NEW MODEL (Flexibility) • Scenario: Rural, remote areas, poor accessibility, poor/limited infrastructure; population of approximately 30,000; multi-culture (Garifuna and Maya predominantly); highest poverty pockets; lowest literacy. • Based on Public Health System. • Apply contractual model with incentives built in. • Monitoring and Evaluation of performance.
LESSONS LEARNED • Turf War. • Perception of privatization • PR/PI Campaign (Marketing NHI) • Institutional strengthening. • Monitoring and evaluation. • Leadership. • Political advocacy • “Window of opportunity”
THE END THANK YOU !!!!!