THYROIDITIS
THYROIDITIS. Inflammatory diseases of the thyroid gland with different etiologic, biologic, histologic and clinical aspects CLASSIFICATION ACUTE: bacterial, viral SUBACUTE: de Quervain’s thryoiditis CHRONIC: chronic autoimmune thyroidits Tuberculous Mycotic

THYROIDITIS
E N D
Presentation Transcript
THYROIDITIS Inflammatory diseases of the thyroid gland with different etiologic, biologic, histologic and clinical aspects CLASSIFICATION • ACUTE: bacterial, viral • SUBACUTE: de Quervain’s thryoiditis • CHRONIC: • chronic autoimmune thyroidits • Tuberculous • Mycotic • Riedel’s thyroidits
ACUTE BACTERIAL THYROIDITIS Signs and symptoms • Fever • Pain profound and severe • Dysfagia - 90 % din cazuri • Dyspnea – 50 % • Spasmodic cough Laboratory data • increased ESR • leukocytosis with neutrophilia • Ultrasound: small or large hypoechoic areas • FNB: isolation of germs Treatment : antibiotics
SUBACUTE ”DE QUERVAIN’S” THYROIDITIS PREVALENTA Sex ratio F/M: 3,6/1 – 10,6 /1 1 caz TS for 5 cases of Graves disease and for 20 cases of AIT • 0,01 % of all hospitalized patients • 1,89 % of all patiens hospitalized for thyroid diseases • 9,9 % of subjects presenting with thyrotoxicosis • 1,52 % of patients investigated by FNB Szabolosz I. Subacute thyroidits Budapesta 2000
SUBACUTE THYROIDITIS ETIOLOGY • probably the disease is a response to a viral infection GENETICS • those with HLA-Bw35 have a risk to develop the disease of 8-56.6 % • HLA-Bw35 allows the development of clincal symtoms • it has no relatioship with the evolution of the disease
SUBACUTE THYROIDITIS PATOGENICITY • interleukine 6 produced by monocytes si macrophages determine inflammation • interleukine 2 +TNF + interferon determine destructive thyroiditis in 10 % of cases • VEGF, basic FGF, PDGF determine granulomatous reaction • EGF determines by mitogenic effect the regeneration of the follicles PATHOLOGY • Follicular disruption with thyroglobulin liberation is responsible for the initial phase of thyrotoxicosis • granuloma: • a center of giant cells surrounded by macrophages • epithelial cells surrounded by a crown of macrophages involved with antigen presentation
Subacute thyroiditis: generalized hypoechogenicity Subacute thyroiditis: patchy hypoechogenicity
SUBACUTE THYROIDITIS scintiscan Color Doppler ultrasound examination
SUBACUTE THYROIDITIS – TREATMENT FORME SEVERE: GLUCOCORTICODS: • Prednisone: 30-40 mg / day at the beginning of the disease with further reduction of the dosage • Dexametazone: 3-4 mg /zi FORME USOARE: Nonsteroidal anti inflammatory drugs: indometacin
AUTOIMMUNE THYROIDITIS INCIDENCE • 3,5 – 4,5 % of population present autoimmune thyroid diseases • 4,6 % of women and 1,23 %of men have antithyroid antibodies • 15 % of women over 60 years • lymphocytic infiltrations: 6,8 5 of women and 2,7 % of men • 50 % of those with antithyroid antibodies have TSH > 6 U.I./ml • 60 % of those with TSH > 6 U.I./ml have antithyroid antibodies • 80 % of those with TSH > 10 6 U.I./ml have antithyroid antibodies • 5 % of those with TSH > 6 U.I./ml develop overt hypothyroidism each year
AUTOIMMUNE THYROIDITIS PATOGENY • genetic predisposition • Viral aggression • excessive iodine supply GENETIC PREDISPOSITION • relatives with autoimmune thyroid diseases • patients with genetic abnormalities :Turner, Klinefelter, Down syndrome • association with other autoimmune diseases: • multiple autoimune endocrine diseases type I and II (ICSR, ovarian failure with precocious menopause ) autoimmune hypophysitis Biermer disease , sd, Sjogren, lupus, rheumatoid arthritis , miastenia gravis, interstitial lung disease • HLA-DR3 si HLA-DR4
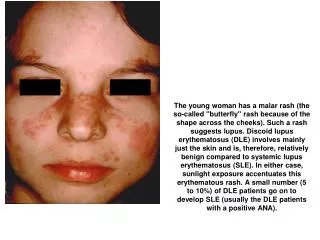
AUTOIMMUNE THYROIDITIS LABORATORY DATA • T4, T3 frequently normal • TSH normal or slightly elevated • increased response of TSH to TRH • anti TPO – ab – 100 % • anti TG-ab – 90 % • TBII – 15-20 % ULTRASOUND EXAMINATION THYROID VOLUME: Increased, normal or decreased Intense hypoechogenicity Scintiscan : patchy hypoechogenicity FNB: lymphocytes and Hurthle cells HASHIMOTO’S thyroiditis • goiter • metabolic state • eutiroidism – 80 % • hipothyroidism – 15 % • hiperthyroidism – 5 % TREATMENT THYROID HORMONES
AUTOIMMUNE THYROIDITIS CLINICAL FORMS • HASHOTOXICOSIS • IN CHILDREN AND ADOLESCENTS: diffuse euthyroid goiter 10-15 % of goiters at these ages • ATROPHIC • SILENT or PAINLESS • POSTPARTUM THYROIDITIS : TPO-Ab are detectable in predisposed cases in the 6th month of pregnancy: hiperthyroid state + depression it occurs postpartum weeks 11-12 and is followed by transient or definitive hypothyroidism • AUTOIMMUNE THYROIDITIS SI MALIGN LYMPHOMA • AUTOIMMUNE THYROIDITIS and THYROID CANCER • IATROGENIC: interpheron, increased iodine intake, external radiotherapy
THYROID NODULES • CLINICAL : 4-7 % (5-20%) • NECROPSIES:40-50 % (30-60%) • ULTRASOUND EXAMINATION 16-67 % CLINICA OF ENDOCRINOLOGY IASI: - MEN : 27,37 % - WOMEN: 30,3 % CHILDREN: 1-2% • THE PREVALENCE INCREASES WITH AGE BY : 0,08 % / year THYROID CANCER: < 10 % OF PALPABLE NODULES, <5 % OF NODULES DETECTED BY US NODULS 4 % OF POPULATION X 4% RISK= POSSIBLE INCIDENCE: 1,6/103 TRUE PREVALENCE : 0.025-0,050/103 1/30 MICROCANCERS BECOME CLINICALY DETECTABLE (MEYER 2000)
THYROID NODULES • CYST • HETEROGENOUS ENDEMIC GOITER • ADENOMA • THYROIDIS • CANCER • LYMPHOMA • EXTRATHYROIDAL LESION
THYROID CANCERS INCIDENCE B/106 F/106 • USA: 2,4-2,8 5,6-6,2 • Australia: 0,7 2,1 • Japan: 1.1 2 • Hawai: 3,1 4 • Germany: 2,7 • USA: ’85-’95: 13.856 cases = 1 % Cancer Data Base Necropsies: Honolulu: 15,16% Hiroshima 25,3 USA: 1,09-1,84 MORBIDITY: NEW CASES /106/ year • SOKAL 1954: 12 / 106/ year • CUTTLER 1975: femei: 52 /106/year barbati: 21/ 106/year • INGBAR 1981: 36 / 106/year • IMPIERI 1984: 10-30 / 106/year • MAZAFFERRY 1988 : 37 / 106/year
Steady increase of thyroid cancer all over the worldBetween 1973-2002 • Mortality decreased from 0.57 to 0.47/105/year • external irradiation stopped after 1961 • precocious diagnosis by ultrasound and FNB • increased incidence but stable mortality • Papillary cancer has a long evolution and excellent survival • 2.4 times increase in thyroid cancer incidence • All thyroid cancer • 3.6/105 8.7/105/year • Papillary cancer • 2.7/105 7.7/105/year • Small papillary cancer • 87 % of the cancer increase
Trends in thyroid cancer • There was noticed steady increase of thyroid cancer all over the world • External irradiation is the only well documented cause in papillary thyroid cancer leading to RET/PTC re-arrangements • Iodine deficiency may play a role in the development of follicular cancer and may favor the development of anaplastic carcinoma • Iodine repletion is associated with increased incidence of papillary carcinoma with excellent prognosis
The ratio of papillary to follicular thyroid cancer (M.Goldust, S.Samankan etc al,2012) (J. D. Cramer, 2010)
Figure 4. Percentage of thyroid cancer operated for each period of 5 years from the entire examined cohort
Etiology and patogeny of thyroid cancers external irradiation: “ ..until now the only carcinogenetic factor for the thyroid in man is external irradiation Duffy si Fitzgerald 1936: firs obsercation of radiatioon induced thyroid cancer in children irradiated for benign lesions of head and neck New cases of thyroid cancer in in Belarus 1990-1995 –Cernobil effect ( Pacini: J.Clin.Endorinol.Metab.1997) 1990 – 31, 1991 – 66, 1992 – 72, 1993 – 94, 1994 – 96, 1995 – 90 78.8 % sub 14 ani Prezumed thyroid cancer: 10- 40 Excess of thryodi cancer due to external irradiation after Cernobil: 200 - 800 Increased susceptibility: Irradiation of head and neck in all children • external irradiation for othe rcancers • Vage less than 20 years • Female sex • Genetic predisposition