Download
1 / 42
450 likes | 1.03k Views
Diabetes and the Eye. Presented to DES chapters by the Canadian Association of Optometrists. Diabetes mortality. Three million Canadians will be living with diabetes by the end of this decade. Diabetes contributes to the death of 41,500 Canadians each year.

E N D
Diabetes and the Eye Presented to DES chapters by theCanadian Association of Optometrists
Diabetes mortality Three million Canadians will be living with diabetes by the end of this decade. Diabetes contributes to the death of 41,500 Canadians each year. Type 2 diabetes shortens life expectancy by 5-10 years.
Diabetes morbidity Diabetes doubles the risk of stroke. Diabetes quadruples the risk of heart disease. Diabetes is the leading cause of non-traumatic lower extremity amputations. Diabetes causes 33% of the new cases of end stage renal disease. Diabetes is the leading cause of blindness in adults aged 25-75.
Components of visual function PSYCHOLOGICAL • visual perception • cognitive functions PHYSICAL PHYSIOLOGICAL • light energy • dioptric system • photoreceptors • neurological processing
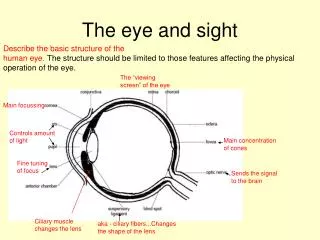
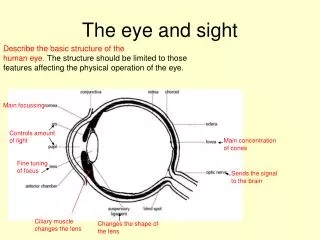
Ocular effects of diabetes 8 1. Cornea + tears 2. Aqueous 3. Iris 4. Lens 5. Vitreous 6. Retina 7. Internal muscles 8. External muscles 7 3 6 1 2 4 5 3 7 8
Ocular effects of diabetes Cornea – hypoesthesia, delayed healing, thickness changes Aqueous – glucose concentration, refractive index changes Iris – neovascularization, secondary glaucoma Lens – refractive changes, cataract development Vitreous – lipid deposits, hemorrhage Retina – edema, ischemia, hemorrhage, neovascularization Intraocular muscles – paresis, accommodative dysfunction Extraocular muscles – paresis, sudden onset diplopia
Fluctuating vision Diabetes can cause large shifts in nearsightedness and farsightedness as blood sugar levels fluctuate
Diabetic lens changes Transient hyperopic refractive changes in newly diagnosed juvenile diabetes. Giusti C. Swiss Med Wkly 2003;133:200–205 Transient refractive changes are highly dependent on the magnitude of plasma glucose concentrations Correction of hyperglycemia is strictly correlated with complete recovery of ocular refraction Sorbitol production via the polyol pathway with overhydration of the lens remains the best pathophysiological hypothesis
Diabetic iris changes Ischemia is thought to initiate retinal & iris neovascularization Vascular endothelial growth factor (VEGF) likely plays a central role in neovascularization New vessel growth at the pupillary border, iris surface and iris angle leads to formation of fibrovascular membranes Membranes in the anterior chamber angle block aqueous outflow causing glaucoma
Canadian Diabetes Association2008 Clinical Practice Guidelines Retinopathy key messages: Screening is important for the detection of treatable disease. Screening intervals for diabetic retinopathy vary according to the individuals age and type of diabetes. Tight glycemic control reduces the onset and progression of sight-threatening diabetic retinopathy. Laser therapy reduces the risk of significant visual loss.
Retinopathy Individuals with type 1 diabetes 100% will have some diabetic retinopathy after 15-20 years of diagnosis
Retinopathy Individuals with type 2 diabetes 20% will have some diabetic retinopathy at the time of diagnosis 50% will have some diabetic retinopathy after 7 years of diagnosis 85% will have some diabetic retinopathy after 15 years of diagnosis
Retinopathy - macular edema Remains the leading cause of vision loss in people living with diabetes Can occur at any time in type 1 and 2
Canadian Diabetes Association2008 Clinical Practice Guidelines Recommendations: 1. In individuals 15 y/o or older with type 1 diabetes, screening and evaluation for retinopathy by an expert professional should be performed annually starting 5 years after the onset of diabetes 2. In individuals with type 2 diabetes, screening and evaluation by an expert professional should be performed at the time of diagnosis of diabetes. The interval for follow-up assessments should be tailored to the severity of the retinopathy. In those with no or minimal retinopathy, the recommended interval is 1-2 years.
Canadian Diabetes Association2008 Clinical Practice Guidelines 3. Screening for diabetic retinopathy should be performed by experienced professionals, either in person or through interpretation of retinal photographs taken through dilated pupils. 4. To prevent the onset and to delay the progression of diabetic retinopathy, people with diabetes should be treated to achieve optimal control of blood glucose. People with abnormal lipids should be considered at high risk for retinopathy.
Canadian Diabetes Association2008 Clinical Practice Guidelines 5. Patients with sight threatening diabetic retinopathy should be assessed by a general ophthalmologist or retina specialist. Laser therapy and/or vitrectomy and/or pharmacologic intervention should be considered. 6. Visually disabled people should be referred for low vision evaluation and rehabilitation.