Download
1 / 1
10 likes | 179 Views
THE EFFECTS OF SPECIAL CLASS PROGRAMS ON CHILDREN WITH MENTAL RETARDATION. İlker Y ılmaz ( 1 ) , Nabile Berktaş ( 1 ) , Özgen Aras ( 2 ) , Mehmet Yanardağ ( 3 ) , Tuba Sevil ( 1 ) , Ferman Konukman ( 4 ) , Bülent Ağbuğa ( 5 ) , Coşkun Bayrak ( 1 ) , Güven Sevil ( 1 )

E N D
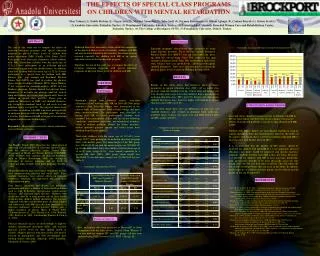
THE EFFECTS OF SPECIAL CLASS PROGRAMS ON CHILDREN WITH MENTAL RETARDATION İlker Yılmaz (1), Nabile Berktaş (1), Özgen Aras (2), Mehmet Yanardağ (3), Tuba Sevil (1), Ferman Konukman (4), Bülent Ağbuğa (5), Coşkun Bayrak (1), Güven Sevil (1) (1) Anadolu University, Eskişehir, Turkey, (2) Dumlupınar University, Kütahya, Turkey, (3) Eskişehir Adult Mentally Retarded Women Care and Rehabilitation Center, Eskisehir, Turkey, (4) The College at Brockport, SUNY,(5) Pamukkale University, Denizli, Turkey. ABSTRACT Study Protocol The aim of this study was to compare the effects of inclusion education programs with special education programs on physical fitness levels of children with mental retardation (MR) (Cuckle, 1999; Beets, 2005). Participants were sixty-nine elementary school students with MR. Thirty-four children with the mean age of 12.3±2.4 were participants in an inclusion physical education program with non disabled peers. In addition, thirty-five children with the mean age of 12.1±1.8 were participants in a special class for children with MR. Balance tests, grip strength and Brockport Physical Fitness Test (BPFT) was used to evaluate the physical fitness levels of children (Winnick, 1999). Mann Whitney U test was used for statistical analysis (SPSS 10.0 for Windows program). Results showed that physical fitness parameters; 20 m shuttle run, push-up, trunk lift, vertical jump and balance test scores were significantly lower in children in special class (p<0.05). There were no significant differences in BMI, calf skinfold thickness, grip strength in dominant hand, sit and reach test and modified Apley test (p>0.05). The physical fitness level was better in children with MR who were participated in an inclusion program with non disabled peers. Therefore, it is better for children with MR to be part of an inclusion program with their non disabled peers. Keyword(s): adapted physical activity, mental retardation exercise/fitness, inclusion Although there have been many studies about the comparison of the physical fitness levels of mentally children with MR and non-disabled children in the literature, there have been no research especially for children with MR in an special education versus inclusion education program. Therefore, the aim of this study was to compare the effects of inclusion education programs with special education programs on physical fitness levels of children with MR. Table 3.Statistically significant differences among observed parameters Education programs’ effectiveness were evaluated by using major outcome measures. These measures include Brockport Physical Fitness Test (BPFT) [16m and 20m shuttle run, push-up, trunk lift, vertical jump (Takei TM), sit&reach test, grip strength in dominant hand (Takei TM) and modified Apley test], static balance tests (eye open/closed), calf-triceps-subscapular skinfold thicknesses. These tests were also used to evaluate the physical fitness levels of children (Winning & Short, 1999) RESULTS METHOD Results of this study shows that children’s physical fitness parameters in special education class (SEC) [20 m shuttle run, push-up, trunk lift, modified curl-up, vertical jump and balance test (eye closed)] scores were lower than children’ fitness parameters in inclusion education class (IEC) (p<0.05). Triceps and subscapular skinfold thicknesses were, however, higher with children in special education class (SEC) (p<0.05). On the other hand, there were no differences in 16m run, calf skinfold thickness, grip strength in dominant hand, sit&reach, modified Apley, balance (eye open) tests and BMI between SEC and IEC groups (p>0.05). Participants Randomly chosen from different schools, sixty-nine elementary school students with MR (in 2005 fall-2006 spring semesters) from Eskisehir, Turkey were investigated in the current study. All participants lived in home settings and none were institutionalized. The participants were classified as having mild MR by school professionals. Students were excluded from participation if they had any of the following conditions: ambulatory limitations, musculoskeletal disorders, visual or auditory problems. Before the fitness measures, written informed parental consent and verbal assent were obtained from all participants. Thirty-four children with the mean age of 12.3±2.4 years (range:10-17) were participants in inclusion education program (IEC) with healthy peers. The mean height of the IEC group was148.62±15.79 cm and the mean weight was 38.88±11.67 kg. On the other hand, thirty-five children with the mean age of 12.1±1.8 years (range:10-16) were trained separately in a special MR class (SEC). SEC group’ mean height was144.26±13.74 cm and mean weight was 39.94±13.69 kg (see Table 1). CONCLUSION & DISCUSSION This study shows that physical fitness levels of children with MR in IEC aremuch higher and their body fat percentages, which cause obesity-related health problems, is much less than children with MR in SEC. Children with MR in Turkey are still educated together in separate schools and classes from their disabled peers. However, the results of the current study found that it is better for children with mild MR to take education with healthy peers (in IEC). It is recommended that the number of IEC classes should be increased for children with mild MR If it is not applicable, physical education class hours should be improved and specific egzercise programs should be used for each child in this class hours. Therefore, it is possible for children with MR to have necessary knowledge, skill, and positive attitudes to be more physically active not only during shool time but also their after-school life. This will reduce the risk of their health problems that can occur in the future. In addition, health expenses of children and their parents can be reduced and the quality of life can be improved. Table 2.Comparison of physical fitness parameters, balance and skinfold thickness on groups. INTRODUCTION The Healthy People 2010 objectives for school physical education indicate that 50% of class time should be spent with the students physically active (United States Department of Health and Human Services [USDHHS], 2000). Children with cognitive and physical disabilities such as Mental Retardation (MR) are willing to participate in exercise programs and are likely to experience many benefits from these programs (Cuckle , 1999). Mental Retardation may cause many limitations in daily vital communication, physical and social skills.These multiple limitations have adverse effects on muscular endurance, education, life expectancy and social skills with family and peers. Poor fitness, inactivity, and obesity can potentially predispose children to a number of future health problems such as type II diabetes, hypertension, cardiovascular diseases, and coronary heart diseases. Children with disabilities may be at even greater risk of these health problems than children without disabilities. For instance, compared with their non-disabled peers, disabled children and adolescents with MR typically have lower levels of muscular endurance,cardiorespiratory fitness and a higher incidence of obesity (Beets & Pitetti, 2005; Chaiwanichsiri et al., 2000; Fernall et al., 1996; Kenneth, 1989; Pitetti et al., 2001; Van Beurden’ Barnett, & Zask et al., 2003) Table 1.Participants’ Characteristics (N=69) REFERENCES Beets, M. W., & Pitetti, K. H. (2005). Contribution of physical education and sport to health-related fitness in high school students. Journal of School Health, 75, 25-30. Chaiwanichsiri et. al. (2000). Poor physical fitness of adolescents with mental retardation at rajanakul school. Bangkok. Journal of the Medical Association of Thailand, 83, 1387-1392. Cuckle P. (1999). Getting in and staying there: children with Down syndrome in mainstream schools.Down Syndrome Research and Practice,6, 95-99. Fernall et al. (1996). Cardiorespiratory capacity of individuals with mental retardation including down syndrome. Medicine and science in sport and exercise, 28, 366-371. Kenneth, F.S. (1989). Pediatric neurology. Mosby company, 115-127. Pitetti et. al. (2001). Cardiovascular fitness and body composition and youthwith and without mental Retardation. Adapted Physical Education Quarterly, 18, 127-141. Schreiber, J., Marchetti, G., & Crytzer, T. (2004). The Implementation of a Fitness Program for Children with Disabilities: A Clinical Case Report. Pediatric Physical Therapy, 16, 173–179. Takeuchi, E. (1994). Incidence of obesity among school children with mental retardation in JaAmerican Journal on Mental Retardation, 99, 283–288. US Department of Health and Human Services. (2000). Healthy People 2010: Physical Activity in Children and Adolescents. Retrieved March 28, 2007 from http://www.healthypeople.gov/Document/HTML/volume2/22Physical.htm Van Beurden, E., Barnett, L. M,, Zask, A.,et al. (2003). Can we skill and activate children through primary school physical education lessons? Move it groove it: a collaborative health promotion intervention. Preventive Medicine, 36, 493–501. Winnick, J. P., & Short, F. X. (1999). The Brockport Physical Fitness Test Manual, Human Kinetics,USA. Statistical Analysis Physical education classes are ideal settings to improve children fundamental movement skills and increase physical activity levels for their optimal health in schools. Adaptive physical education classes also may be focused on participation and skill development than lifelong fitness education (Takeuchi, 1994; Schreiber, Marchetti, & Crytzer, 2004). First, description data were presented as Means±SD to allow comparison with the other results. Second, Mann Whitney U test was used for compare IEC and SEC groups. All data were analyzed using SPSS (version 10.0.0; SPSS, Chicago, IL).