Download
1 / 31
310 likes | 499 Views
Assessment of Ocular Injury and Visual Function in Veterans with TBI from Combat Blast Glenn Cockerham, MD VA Palo Alto Health Care System Palo Alto, California. Presentation Goals. Blast effects on the eye and visual function

E N D
Assessment of Ocular Injury and Visual Function in Veterans with TBI from Combat Blast Glenn Cockerham, MD VA Palo Alto Health Care System Palo Alto, California
Presentation Goals • Blast effects on the eye and visual function • Assessment of eye injury in subjects with traumatic brain injury (TBI) from blast • Testing of visual function
Financial Disclosures • NONE
Acknowledgements • Travel support from DoD/VA Vision Center of Excellence • Funding support from the Veterans Health Administration by Merit Review Award C5018R
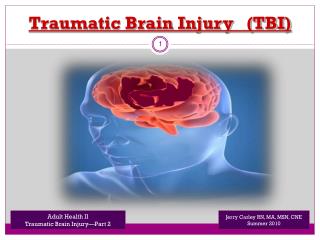
TBI and Blast • Blast most common cause of TBI in Iraq and Afghanistan • In 2008 over 300,000 potential TBIs from blast estimated by RAND Corporation, out of 1.2 million U.S. military who had served in Iraq • Incidence of closed-globe ocular injury and visual dysfunction unknown • Okie S. Traumatic brain injury in the war zone. N Engl J Med 2005;352:2043-2047.
Blast and The Eye • Blast forces severe enough to cause TBI may injure the eye, adnexa (eyelids), orbit, and optic nerve • Eye is vulnerable to frontal (and other vectors?) overpressure, stress waves and shear waves • Visual dysfunction possible from eye, optic nerve or central damage
Anatomic Evaluation of the Eye after Blast Injury • Ocular examination • CT imaging of orbital bones, optic canal • MRI of visual pathways, brain • Retinal nerve fiber layer by spectral domain optical coherence tomography (OCT) • Corneal endothelium density and morphology by specular microscopy
Ocular Examination • Closed-globe injury: external or internal damage to eye without penetration or rupture of eye wall • Examination visualizes all compartments and tissues of eye • Ocular trauma classification divided into anatomic zones • Pieramici DJ, et al. A system for classifying mechanical injuries of the eye (globe). Am J Ophthalmol 1997;123:820-831.
Closed-globe Ocular Injury in Blast • 43% of 46 subjects with blast TBI had closed-globe ocular injury • No evident protective effect from ballistic eyewear (W = 246.5, Z = -.54, p = .64) • Visual acuity not predictive of ocular injury (chi-square = 2.39, p= 0.15) • Cockerham GC, et al. Closed-eye ocular injuries in the wars in Iraq and Afghanistan. N Engl J Med 2011;364:2172-2173.
Extensive orbital fractures, right orbital hemorrhage with no light perception
23 Year Old Marine, Right IED Blast, Ballistic Eye Wear: Endothelial Cell Density by Specular Microscopy Right eye, CD 1207 Left Eye, CD 2681
Tests of Visual Function • Psychometric tests • Require attention and cooperation • Visual acuity • Contrast sensitivity • Visual fields • Accommodation (focus) • Color discrimination
Visual Acuity • Worldwide test for vision for > 100 years • Traditionally measured with high-contrast Snellen optotypes • 20/20 or 6/6 notation • Gold standard for clinical testing and research ETDRS Chart 100% Contrast
Visual Acuity: What does it measure? • Spatial limit of visual resolution • Normal minimal angle of resolution is 30 seconds arc • Requirements for optimal vision: • Photopic conditions • Clear optical media • Steady foveal fixation • Intact photoreceptors • Intact afferent visual pathways
Limitations to Standard Visual Acuity Testing • Uses 100% contrast targets (not real world scenario) • Not sensitive to subclinical disorders affecting afferent pathways • May be normal in neuro-ophthalmic conditions, such as multiple sclerosis (MS)
Low-Contrast Visual Acuity (LCVA) in Multiple Sclerosis • Correlations with LCVA • T2 lesion volume (3-mm3 increase per line of vision) • OCT RNFL (4 micron decrease per line of vision) • Functional scales (EDSS – expanded disability status scale) 2.5% Contrast Balcer LJ, Frohman EM. Evaluating loss of visual function in multiple sclerosis as measured by low-contrast letter acuity. Neurology 2010;74:S16-S23.
High-Contrast Visual Acuity in Blast TBI • 55 examinations at baseline • 62% were 20/20 or better in both eyes • 21% had one eye between 20/25 and 20/40 • 17% had one eye worse than 20/40
Spatial Contrast Sensitivity (CS) • Light-dark transition at edge of object • Contrast is ratio of difference in luminance between areas (0%= no contrast) • In CS testing the contrast is varied to determine the threshold (unlike visual acuity, in which the contrast remains the same and the target size varies)
Contrast Sensitivity Grating Tests • Sine wave grating patches • Illuminated cabinet • Different spatial frequencies • 3,6,12,18 cycles per degree
Spatial Contrast Sensitivity in TBI • 47 tests at baseline examination • 47% had CS reduced by 2 SD in at least one eye
Automated Perimetry • Tests sensitivity of the visual field • Each point on the retina is represented in visual space and can be tested • Peak sensitivity in the center of retina (fovea) and decreases towards periphery
Visual Field Testing in TBI • Main concern is test duration: full-threshold testing takes about 12 minutes per eye • Swedish Interactive Threshold Algorithm (SITA): reduces testing time by half (6 minutes) • Frequency-doubling technology (FDT): uses flicker target instead of stationary white stimulus, reduces screening test time to 2 to 3 minutes
Automated Static Perimetry with SITA Algorithm Field Depression (Decreased Sensitivity) Complete Hemianopia of Left Visual Field
Automated Static Perimetry in TBI • 49 reliable tests at baseline examination • 63% had significantly reduced mean deviation (reduced field sensitivity) in at least one eye • 8 had neurologic scotomas (4 hemianopias, 4 quadrantanopias)
Accommodation • Dynamic change in lens curvature to allow focus on near targets • Accommodative triad: accommodation, convergence, and miosis (pupil constriction) • Preoccipital cortex, midbrain, oculomotor nuclei • Subjective symptoms include eye pain, headache, difficulty with near vision, diplopia
Accommodative Testing Open Field Analyzer Accommodative Rule
Summary • Blast forces may damage eyes and visual pathways • Visual function, especially visual acuity, may be relatively normal • Further research required for best practices in detecting damage and dysfunctions
Team Members • Thomas Rice, MD • Sonne Lemke, PhD • Kimberly Cockerham, MD, FACS • Eva Hewes, MD • Richard Lin, MD, PhD • Gloria Wang, MD • Catherine Glynn-Milley, RN, CRNO • Lars Zumhagen, MD