Download
1 / 37
370 likes | 443 Views
This workshop explored the integration of meta-analysis results into evidence-based decision modeling processes. Key topics included pooled estimates, transforming distributions, and common modeling issues. Examples like the Net Clinical Benefit Approach were discussed. The use of Bayesian methods, random effect meta-analysis models, and WinBUGS software was emphasized to handle uncertainty in parameter values. Highlighting the re-analysis of Warfarin for non-rheumatic atrial fibrillation, the workshop illustrated how to evaluate trade-offs between stroke and hemorrhage risks in terms of quality of life. Various sources of evidence, including multivariate risk equations and quality of life studies, were compared to calculate the net benefit in stroke equivalents. Practical insights and methodologies were shared to guide decision-making processes.

E N D
The Incorporation of Meta-Analysis Results into Evidence-Based Decision Modelling Nicola Cooper, Alex Sutton, Keith Abrams, Paul Lambert, David Jones Department of Epidemiology & Public Health, University of Leicester. CHEBS, Multi-Parameter Evidence Synthesis Workshop, Sheffield, March 2002
Where we fit in with Tony’s intro • Process • Model relationship between evidence & parameters • Consistency check • Uncertainty Panacea • Statistical error • ½ Evidence relates to parameters indirectly • Systematic errors • Data quality, publication bias, etc
METHODOLOGIC PRINCIPLE 1) Pooled estimates
METHODOLOGIC PRINCIPLE 1) Pooled estimates • 2) Distribution
METHODOLOGIC PRINCIPLE 1) Pooled estimates • 2) Distribution 3) Transformation of distribution to transition probability (if required) (i) time variables: (ii) prob. variables:
METHODOLOGIC PRINCIPLE 1) Pooled estimates • 2) Distribution 4) Application to model 3) Transformation of distribution to transition probability (if required) (i) time variables: (ii) prob. variables:
EXAMPLES • Net Clinical Benefit Approach • Warfarin use for atrial fibrillation • Simple Economic Decision Model • Prophylactic antibiotic use in caesarean section • Markov Economic Decision Model • Taxane use in advanced breast cancer
MODELLING ISSUES COMMON TO ALL EXAMPLES • Bayesian methods implemented using Markov Chain Monte Carlo simulation within WinBUGS software • Random effect meta-analysis models used throughout • All prior distributions intended to be ‘vague’ unless otherwise indicated • Where uncertainty exists in the value of parameters (i.e. most of them!) they are treated as random variables • All analyses (decision model and subsidiary analyses) implemented in one cohesive program
EXAMPLE 1: NET (CLINICAL) BENEFIT Net Benefit = (Risk level x Risk reduction) – Harm • Glasziou, P. P. and Irwig, L. M. An evidence based approach to individualizing treatment. Br.Med.J. 1995; 311:1356-1359.
RE-ANALYSIS OF WARFARIN FOR NON-RHEUMATIC ATRIAL FIBRILLATION • Evidence that post MI, the risk of a stroke is reduced in patients with atrial fibrillation by taking warfarin • However, there is a risk of a fatal hemorrhage as a result of taking warfarin • For whom do the benefits outweigh the risks?
METHOD OUTLINE • Perform a meta-analysis of the RCTs to estimate the relative risk for benefit of the intervention • Use this to check the assumption that RR does not vary with patient risk • Check harm (adverse events) is constant across levels of risk (use RCTs and/or data from other sources) & estimate this risk • Place benefit & harm on same scale (assessment of QoL following different events) • Apply model - need to predict patients risk (identify risk factors and construct multivariate risk prediction equations)
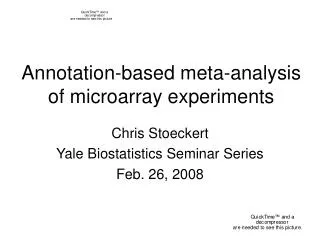
SOURCES OF EVIDENCE Net Benefit = (risk of stroke x relative reduction in risk of stroke) - (risk of fatal bleed x outcome ratio) Multivariate risk equations M-A of RCTs M-A of RCTs/obs studies QoL study
Singer,D.E. Overview of the randomized trials to prevent stroke in atrial fibrillation. Ann Epidemiol 1993;3:567-7.
EVALUATING THE TRADE-OFF BETWEEN STROKE AND HEMORRHAGE EVENTS IN TERMS OF QOL • QoL following a fatal bleed = 0 • Data available on QoL of patients following stroke • Glasziou, P. P., Bromwich, S., and Simes, R. J. Quality of life six months after myocardial infarction treated with thrombolytic therapy. The Medical Journal of Australia. 1994; 161532-536 Proportion with index greater than horizontal axis value Time trade-off index
10 6 8 6 4 4 2 2 0 0 -2.95 -2.90 -2.85 -2.80 -2.75 -2.70 -2.65 -1.5 -1.0 -0.5 0.0 0.5 1.0 reduction in relative risk 300 250 0.4 200 150 0.3 100 0.2 50 0.1 0 0.002 0.004 0.006 0.008 0.010 0.012 0.014 0.0 risk of bleed per year 0 20 40 60 80 100 Outcome ratio Multivariate Risk Equation Data Net Benefit (measured in stroke equivalents) No. T hrombo - Clinical No. of % of embolism Mean Median Probability of risk patients cohort rate (% (s.e.) (95% Benefit > 0 Simulated PDF factors per year CrI) (95% CI)) 6 5 4 2 or 3 68 12 17.6 (10.5 - 0.0004 0.06 54.2 % 3 to 29.9) (0.15) ( - 0.29 to 2 0.20) 1 0 -0.8 -0.6 -0.4 -0.2 0.0 0.2 0.4 2 or 3 Clinical factors EVALUATION OF NET BENEFIT Risk of stroke Relative risk per year e.g. reduction for for 1 or 2 clinical strokes taking risk factors: warfarin (1 - RR): 6.0% (4.1 to 0.23 (0.13 to 0.41) 8.8) Multivariate risk Meta - analyses equations of RCTs ´ (risk of stroke relative reduction in risk of stroke) - ´ (risk of fatal bleed outcome ratio) = Meta - Analysis of Net Benefit QoL study RCTs / obs studies Outcome ratio (1/ QoL Risk of fatal reduction) Median bleed per 3.75 (1.07 to 50), year taking Mean 26.14,indicating warfarin : the number of strokes 0.52% (0.27 that are equivalent to to 0.84) one death
“TAKE-HOME” POINTS 1 • Net-benefit provides a transparent quantitative framework to weigh up benefits and harms of an intervention • Utilises results from two meta-analyses and allows for correlation induced where studies included in both benefit and harm meta-analyses • Credible interval for net benefit can be constructed allowing for uncertainty in all model parameters
EXAMPLE 2: SIMPLE DECISION TREE • Use of prophylactic antibiotics to prevent wound infection following caesarean section
METHOD OUTLINE • Cochrane review of 61 RCTs evaluating prophylactic antibiotics use for caesarean section • Event data rare: use “Exact” model for RR • Meta-regression: Does treatment effect vary with patients’ underlying risk (pc)? ln(RRadjusted ) = ln(RRaverage)+ [ln(pc) - mean(ln(pc))] • Risk of infection without treatment from ‘local’ hospitaldata (p1) • Derive relative risk of treatment effect for ‘local’ hospital (using regression equation with pc=p1) • Derive riskof infection if antibiotics introduced to ‘local’ hospital (p2) p2 = p1 * RRadjusted
UNDERLYING BASELINE RISK =0.24 (-0.28 to 0.81) No treatment effect Local hospital event rate
Mean (95% Credible Interval) Posterior distribution Relative Risk, RRadjusted 0.30 (0.21 to 0.40) Prob(wound infection/placebo), p1 0.08 (0.06 to 0.10) Prob(wound infection/antibiotics),p2 0.02 (0.015 to 0.034) RESULTS
Mean (95% Credible Interval) Posterior distribution Reduction in cost using antibiotics -£49.53 (-£77.09 to -£26.79) Number of wound infections avoided using antibiotics per 1,000 53.09 (42.12 to 73.37) Between study variance (random effect in M-A), 2 0.30 (0.05 to 0.74) RESULTS (cont.) RESULTS
COST-EFFECTIVENESS PLANE Treatment more effective & more costly Control dominates Treatment less effective & less costly Treatment dominates
SENSITIVTY OF PRIORS [1] Gamma(0.001,0.001) on 2 [2] Normal(0,1.0-6) truncated at zero on [3] Uniform(0,20) on
“TAKE-HOME” POINTS 2 • Incorporates M-A into a decision model adjusting for a differential treatment effect with changes in baseline risk • Meta-regression model takes into account the fact that covariate is part of the definition of outcome • Rare event data modelled ‘exactly’ (i.e. removes the need for continuity corrections) & asymmetry in posterior distribution propogated • Sensitivity of overall results to prior distribution placed on the random effect term in a M-A
EXAMPLE 3: USE OF TAXANES FOR 2ND LINE TREATMENT OF BREAST CANCER Stages 1 & 2 (cycles 1 to 3) Treatment cycles Stage 3 (cycles 4 to 7) Stage 4 (cycles 8 to 35) Post -Treatment cycles
METHOD OUTLINE • Define structure of Markov model • Identify evidence used to inform each model parameter using meta-analysis where multiple sources available • Transform meta-analysis results, where necessary, into format required for model (e.g. rates into transition probabilities) • Informative prior distributions derived from elicited prior beliefs from clinicians • Evaluate Markov model
METHODOLOGIC PRINCIPLE 1) Pooled estimates • 2) Distribution 4) Application to model 3) Transformation of distribution to transition probability (if required) (i) time variables: (ii) prob. variables:
ELICITATION OF PRIORS e.g. Response Rate Taxane Standard
“TAKE-HOME” POINTS 3 • Synthesis of evidence, transformation of variables & evaluation of a complex Markov model carried out in a unified framework (facilitating sensitivity analysis) • Provides a framework to incorporate prior beliefs of experts
FURTHER ISSUES • Handling indirect comparisons correctly • E.g. Want to compare A v C but evidence only available on A v B & B v C etc. • Avoid breaking randomisation • Necessary complexity of model? • When to use approaches 1,2,3 above? • Use of predictive distributions • Necessary when inferences made at ‘unit’ level (e.g. hospital in 2nd example) rather than ‘population’ level? • Incorporation of EVI
MODEL SPECIFICATION Bayesian random effects M-A model specification: ln(RR) Prior distributions: Warn et al 2002 Stats in Med (in press)