Download

1 / 52
590 likes | 1.17k Views
APPROACH TO THE PATIENT WITH HEADACHE. Corey Heitz, MD Jonathan Singer, MD Wright State University School of Medicine. WHY HEADACHE DISCUSSION?. Frequency that problem is seen Example: H&P central to evaluation Potential for morbidity, mortality Identification may prevent sequelae.

E N D
APPROACH TO THE PATIENT WITH HEADACHE Corey Heitz, MD Jonathan Singer, MD Wright State University School of Medicine
WHY HEADACHE DISCUSSION? • Frequency that problem is seen • Example: H&P central to evaluation • Potential for morbidity, mortality • Identification may prevent sequelae
CONTENT OF DISCUSSION • Nontraumatic acute through chronic • Pathophysiology of pain perception • Provide few classification systems • Emphasis toward the catastrophic
FURTHER CONTENT • Clues from history, physical • Role of diagnostic adjuncts • Influence of age, sex • Goals of individual encounter
PERCENTAGES WITH HEADACHE • 80% of population in any year • 45% early, 75% late adolescence • 99% develop within their lifetime • Most accept as “human cond”
HEADACHE, PHYSICIAN VISIT • Not all patients seek doctor • We possess different behaviors • Treatment seeking for acute, chronic • 4-10% see doctor episodically
STAGGERING HEALTH EFFECTS • Number 1 chronic ED problem • 9th among ambulatory complaints • 1-2% of E.D. chief complaints • 200 million missed work days • Billions in OTC, other remedies
HEADACHE DEFINED • Headache typically refers to any head pain including pain in the face, neck, and ears but is generally used to describe pain perceived in the scalp and cranium.
PAIN SENSITIVE STRUCTURES • Scalp epidermis to periosteum • Venous sinuses and branches • Dura mater, arterial supply • Cranial nerves; not parenchyma
INCITORS OF STIMULUS • Mechanical Chemical Metabolic • Mass occupying Chinese Hypoxia,C.O. • Inflammatory Hot dog Withdrawal • Infections Hangover Hypoglycemia
PATHWAYS TO PAIN • Location Pain Pathway • Supratentorial Fore temple 1 div of V • Infratentorial Neck, occip IX, X, C1-3 • Ant cranium Front, glob 3 div of V • Post cranium Front, glob C1-3
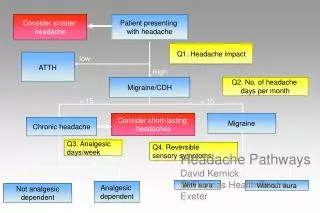
CLASSIFICATION • By temporal pattern • By pathophysiology • By “how urgent”
TYPES BY TEMPORAL PATTERN Acute Acute, recurrent Chronic non-progressive Headache severity Chronic progressive 0 30 60 Time (days)
TYPES BY PATHOPHYSIOLOGY • Vascular Organic Functional • Migraine Mass lesion Tension • Cluster ICP Depression • Toxic ICP Conversion Rx
TYPES BASED ON THREAT • Emergent Urgent Benign • I.C. Bleeding Vascular Tensions • ABM, aseptic Mass Medications • Hypertension Systemic Heent inf • Oxygenation Glaucoma
BENIGN HEADACHES • Overwhelming majority causes benign • 90% evaluated in an Emergency Dept. • 33% of pediatric causation, AF illness • “Benign” still debilitating, alarming
CHALLENGES OF ENCOUNTER • Identify if an ominous cause • Deliver any emergent interventions • Offer your diagnosis and relief • Arrange appropriate F/U care
PAIN: IMPORTANCE OF DATA • Quality Manipulation • Onset Prodromal events • Location Associated symptoms • Duration Family history • Medications Past med history
QUALITY OF HEADACHE • Stabbing: trig neural, arteritis,herpes • Boring: withdrawal, cluster, sinusitis • Aching: tension, enceph, meningitis • Throbbing: migraine, BP, TIA, CVA
PRECIPITATION OF HEADACHE • Migraine and cluster have precipitants • Dairy, legumes, red wines (tyramine) • Chocolate, nitrates, and MSG • Premenstrual, stress, weather change
ONSET OF HEADACHE • Sudden: SAH, tumor with bleed • Exertional: SAH • Worse am: BP, brain tumor • Worse pm: cluster headaches • Awaken: BP, SAH, tumor
LOCATION OF HEADACHE • Frontal: TIA, CVA, arteritis • Vertex: tension • Occipital: tension, toxic, BP • Generalized: pyrexia, toxic • Hemi: migraine, CVA, arteritis, cluster
DURATION OF HEADACHE • No duration entirely predictive • Acute: toxic, noncephalic infection • Subacute: cluster, tumor • Chronic: neuralgias, migraine
MEDS: DRUG INDUCED • BP: amphet, cocaine, phenylephrine • Dilatation: nitroglycerine • ICP: steroid, tetracycline, retinoids • Cran nerve irrit: ergot, MAO inhibitors • Unknown: birth control pills
PURSUING CHEMICAL TRIGGERS • Inquire re Rx, OTC’s, illicit drug use • Caffeine use, seeking withdrawal • Topical anesthetics (methemoglobinemia) • Methylene chloride (CO), acetonitrile (cyanide) • Mahuang (ephedra), hypervitaminosis
PAIN: IMPORTANCE OF DATA • Quality Manipulation • Onset Prodromal events • Location Associated symptoms • Duration Family history • Medications Past med history
MANIPULATIONS FOR HEADACHE • Pace, rock, head butt think cluster • Rhythmic rubs of contraction, migraine • Torticollis, avoid valsalva - ICP • No speech, sound, light of migraine
PRODROMAL SCREENING • Recent trauma, even if “minor” • When severe seek sentinel bleed • Paraesthesias or altered mood • Premonitory motor or visual aura
MIGRAINEURS AURA • Flashing lights (photopsia) • Bright wavy lines (teichopsia) • Shimmering zig zag (s. scotoma) • Blindness for 1/2 field (hemianopsia) • Size distortion, Alice (metamorphopsia)
PAIN: IMPORTANCE OF DATA • Quality Manipulation • Onset Prodromal events • Location Associated symptoms • Duration Family history • Medications Past med history
HEADACHE WITH “FLU” • Fever: intracranial, extracranial infection • Malaise, myalgia: meningitis, CO, arteritis • A,N,V: arteritis, migraine, BP, glaucoma • Photophobia: ABM, aseptic, migraine, SAH
HEADACHE PLUS HEENT • Eye pain: glaucoma, sinusitis, thrombosis • Jaw pain: arteritis, MI with CVA • Lacrimation, rhinorrhea of cluster • Neck stiffness: meningitis, SAH • Opthalmoplegia: tumor, AVM, thrombosis
HEADACHE WITH NEUROLOGIC • Presyncopal, syncopal suggests SAH • Hyperesthesia: focal with neuralgias • Paresis: CVA, subdural, tumor, migraines • Aphasia: migraines, CVA, toxic • Ataxia, nystagmus of cerebellar lesions
KEY FAMILY HISTORY • SAH - 4x risk general population • Depression states hereditary • Hypertension, diabetes, atherosclerosis • Cluster 7%, migraine from 60-90%
PMH FOR HEADACHE • Infectious: exp contagion, 1o focus • Endocrine: thyroid, adrenal, BS • Systemic: BP, coag, alcoholism • Diagnostics: anemia, LP, neuroimaging
WHEN BENIGN PMH HEADACHE • When was diagnosis established? • How firm is existing diagnosis? • Have circumstances since changed? • Is there a change in this episode?
GENERAL EXAMINATION • General: acute or chronically ill • Febrile: focal, CNS infect, SAH • RR: metabolic, hypoxia, CO • HR: may reflect pain intensity
HEENT REWARDS • Visual: lacrimation, rhinorrhea, sweating • Auscultation: machine bruit of AVM • Percussion: dental pathology, sinusitis • Palpation: carotid dissect, scalp tender
HIGH YIELD OCULAR • Finding Disease • Ptosis, miosis Cluster • Clouding, mydriasis Glaucoma • Opthalmophegia Sinusitis, tumor • Papilledema ICP • acuity Glauc, arteritis • Hemorrhage BP, SAH
NEUROLOGIC FINDINGS • AMS: Bleed, infection, tumor, migraine • Ataxia, clumsiness, nystagmus, plantar • Weakness in face, limbs or asymmetry • Nuchal rigidity: CNS infection, SAH • Loss of speech: mass lesion or CVA
AT THE END OF H&P • Valued tools for patient stratification • Distinguish emergent, urgent, nonurgent • Does the exact diagnosis matter? • Does scenario warrant diagnostics?
DIAGNOSTICS FOR HEADACHE • Imaging: Sinus films, CT, MRI • Phlebotomy: CBC, ESR, BIood sugar, Carboxyhgb, chemistries • Other: EEG, lumbar puncture
DIAGNOSTIC TESTING MODALITIES • Most headaches are of benign origin • Most require reassurance, analgesia • No “hard rules” by evidence based • Several scenarios are higher yielding
HIGHER YIELD SCENARIOS • History Physical • First, worse Febrile • New after 50 Meningeal signs • New with Ca Mental status • Change pattern Other neurologic • Seizure Focal deficit
IMPACT OF AGE • Childhood Adult • Brain tumor < 7 Brain tumor >50 • SAH rarity Mean SAH, 50 • Lead exposure Coexisting med • Occult injury Drug seeking
IMPACT OF AGE, SEX • Disease prevalence peak variations • Age reduces exhaustive differential • Gender may falsely bias differential • Serious infections bimodally distributed
CASE • 7-year-old with abrupt visual change, • nausea, retroorbital headache. • Neurologic exam normal. Positive • maternal history of migraine.
GOALS FOR FIRST HEADACHE • Family Physician • Pain relief Complete H,P • What’s wrong Classify risk • Is serious Diagnostics • Will recur Diagnosis
CASE • 28-year-old grad student with • worsening bandlike tightness posteriorly. • Frequency, severity affecting academics • and relationships.