Economic and Medical Impacts of National Policy on Highly Resistant Micro-organisms
This study analyzes the economic and medical consequences of stringent national policies aimed at controlling the spread of highly resistant microorganisms (HRM) such as GRE and CPE in hospitals. Evaluating data from a 1000-bed university hospital, the research highlights the increased length of hospital stays, estimated at an extra 22 days and associated costs averaging €6,981 per patient. The findings underscore the balance needed between infection control and patient care, calling for further evaluation in larger, multicenter studies to refine these approaches.


Economic and Medical Impacts of National Policy on Highly Resistant Micro-organisms
E N D
Presentation Transcript
Economic and medicaladverse effects of a national policy to control the spread of highly-resistant micro-organisms. G Birgand a, M Schwarzinger b, A Perozziello c, C Pelat b, L Armand-Lefevre, E Ruppé d, JC Buzzi c, A Andremont d , Y Yazdanpanah b, JC Lucet a aInfection control unit, Bichat-Claude Bernard Hospital, Paris, France bATIP-Avenir, Inserm U738, Paris, France; c Medical Infomation Systems Program (PMSI), Bichat-Claude Bernard Hospital, Paris, France; dBacteriology laboratory, Bichat-Claude Bernard Hospital, Paris, France
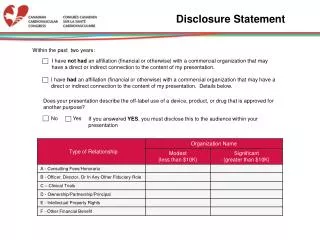
G. Birgand Disclosure statement Financial support: none Conflict of interest: Pfizer: Travel grant for the ICAAC 2011 ECCMID Berlin 2013
G. Birgand IntroductionEpidemiological context GRE CPE E.Faecium VR EARSS 2011 Kp Carba-R EARSS 2011 ECCMID Berlin 2013
G. Birgand Introduction French National Recommandations Patients detected colonised with GRE or CPE: • Single room + contact precautions for carriers and contact patients along the entire hospital stay • Cohorting of carriers and contact patients in 2 different dedicated areas with dedicated staff 24/7 • Interruption of transfers of carriers and contact patients +interruption of new admissions • Repeated rectal sampling of contact patients: D0, D7, D15 ECCMID Berlin 2013
G. Birgand Introduction Potential consequences of guidelines • Medical impact: • Unintended deleterious adverse effects for patients ? • Disruption for the ward • Delays in patient’s care and transfer • Economical impact: • Lost income due to interruption of transfers and admissions (French daily incomes for 1 hospital day: € 300-400 in medical units to € 1700 - 2000 in ICU) • Cost of lab techniques and contact precautions • Cost of additional staff for cohorting ECCMID Berlin 2013
G. Birgand Objectives • Patients colonised with GRE or CPE € Length of stay • Characteristics of hospital stays • The additional • hospital costs From 01/2009 to 06/2012 (3.5 years) in a 1000-bed University Hospital 6 ECCMID Berlin 2013
G. Birgand MethodsStudy design Cases Patient colonised or infectedwithGRE or CPE Controls Patient neveridentified as colonizedwith GRE or CPE Matchingcriteria: gender, ward, period of hospitalisation (n-1), Age, diagnosis-related group (DRG) • Outcomes: • Length of hospital stay and overall hospital cost • Retrospective data collection: • Clinical, microbiological and hospital stay characteristics • Estimated costs of inpatient care based on reimbursement rates of the DRG (national yearly survey, 2011) • Statistical analysis: • Univariate and multivariate ANOVA (SAS and Stata v10)
G. Birgand MethodsStudy population • 37 Pts identified colonised during the study period: • 4 death • 7 still hospitalised 107 surviving patients 26 cases colonised 81 Controlsneveridentified 1 1 18 6 14 GRE 12 CPE 10 vanA 4 vanB 9 OXA-48 2 KPC 1 NDM-1 ECCMID Berlin 2013
G. Birgand ResultsDescription of cases
G. Birgand ResultsUnivariate analysis (1) Characteristics Cases N= 26 (%) Controls N= 81 (%) P Age, median (IQR) 65 (57-77) 65 (56-77) 0.84 Female 11 (42) 33 (41) 0.89 Diagnosis-related group 1.00 Respiratory diseases 9 (35) 28 (35) Diabetes 3 (12) 8 (10) Vascular diseases 4 (15) 20 (24) Infectious diseases 3 (11) 9 (11) Others 7 (27) 16 (20) Charlson score, median (IQR) 6 (4-7) 4 (3-6) 0.1 Mc Cabe score 0.55 0 7 (27) 28 (36) 1 17 (65) 42 (53) 2 2 (8) 9 (11) Ward at the time of identification 0.73 ICU 5 (19) 15 (19) Medical unit 15 (58) 53 (65) Surgical unit 6 (23) 13 (16)
G. Birgand ResultsUnivariate analysis (2) Characteristics Cases N= 26 Controls N= 81 P • Median length of stay 28 (12-94) 11 (8-18) <0.01 • Ward at hospital discharge 0,05 • Intensive care unit 0 0 • Surgical ward 9 (35) 27 (33) • Medical ward 14 (54) 53 (65) • Rehabilitation 3 (12) 1 (1) • Destination at discharge • Home 23 (88) 68 (84) 0.57 • Transfer 3 (12) 13 (16) • Health insurance beneficiaries 18 (69) 67 (83) 0.32 • Mean cost of hospitalisation, € (sd) 15,830 (4,320) 8,919 (2,447) <0.01
G. Birgand ResultsMultivariate analysis • Final multivariate mixed models of ANOVA: Excess of length of stay = 22 days (12 - 34) Extra cost = 6,981€ (3,377 – 10,585) ECCMID Berlin 2013
G. Birgand Discussion - Conclusion • The impact of stringent measures to control HDRB on hospital stays characteristics was estimated to: • 22 days (12-34) of mean excess LOS per Pt • 6,981€ (3,377 – 10,585) of mean extra costs per Pt • Strengths of this study: • Matching on patients comorbidity and DRG Most costs are attributable to GRE or CPE • Limits of this study: • Single center study • Costs based on DRG and not individual data. • Perspectives: • Evaluation on a larger population at a multicenter level