Download

1 / 45
0 likes | 10 Views
This presentation focuses on the intersection of substance use disorders, mental health issues, and traumatic brain injuries, highlighting the challenges and missed opportunities in treating individuals with TBI. It covers the public health emergency of opioid crisis, various initiatives, partnerships, and evidence-based approaches to combat the crisis, with a special emphasis on the work of the ACL Opioid and Mental Health Concerns Workgroup. The objectives include raising awareness, sharing best practices, and developing tools to support TBI populations with SUD.

E N D
Traumatic Brain Injury and Substance Use Related Disorders: Building Supports With Our Community Partners Presenter: Gabriela Lawrence-Soto, Massachusetts ACL Opioid and Mental Health Concerns Work Group March 8, 2019 - West Virginia Traumatic Brain Injury Conference

Disclaimer This project was supported, in part by members of the ACL Opioid and Mental Health Concerns Workgroup grant numbers 90TBSG0034-01-00 (Indiana), 90TBSG0029-01-00 (Kentucky), 90TBSG0033-01-00 (Massachusetts), 90TBSG0027-01-00 (Maryland), 90TBSG0042-01-00 (North Carolina), 90 TBSG0035-01-00 (Virginia), and 90TBSG0038-01-00 (West Virginia), from the U.S. Administration for Community Living, Department of Health and Human Services, Washington, D.C. 20201. Grantees undertaking projects with government sponsorship are encouraged to express freely their findings and conclusions. Points of view or opinions do not, therefore, necessarily represent official ACL policy.
Objectives • The Public Health Emergency • What is the Opioid and Mental Health Concerns Work group? • SUD-TBI Prevalence and Intersections • Barriers to Treatment for TBI populations • Highlight Missed opportunities • Partnerships Models used to address the SUD continuum of Care
The Public Health Emergency In 2017 overdose-related deaths were 6 times higher than 1999 President Trump declared the Opioid Crisis a National Public Health emergency Five-point Strategy to combat the Opioid Crisis 1. Better Substance Use Disorder Prevention, Treatment and Recovery Services 2. Better Data 3. Better Pain Management 4. Better Targeting of Overdose Reversing Drugs 5. Better Research Source:
Grant $$ to Combat the Crisis Center for Disease Control and Prevention (CDC) • Prescription Drug Overdose: Prevention for States (PfS) • Prescription Drug Overdose: Data-Driven Prevention Initiative (DDPI) • Enhanced State Opioid Overdose Surveillance (ESOOS) Health and Resource Services Administration (HRSA) • Expanding Access to Quality Substance Use Disorder and Mental Services • Behavioral Workforce Education and Training And Enhancing Behavioral Health Workforce awards • Rural Communities Opioid Response Program-Planning Substance Abuse and Mental Health Services Administration (SAMHSA) • Medication Assisted Program - Prescription Drug And Opioid Addiction (MAT-PDOA) • State Target Response to the Opioid Crisis Grants (Opioid-STR) • Opioid State Target Response Supplement grant (STR Supplement) • Opioid State Targeted Response Technical Assistance (STR TA) • Partnerships for Success (PFS) • First Responders - Comprehensive Addiction and Recovery Act (FR CARA)
Grant $$ to Combat the Crisis …Continued Bureau of Justice Administration • Comprehensive Opioid Abuse Site-based Program (COAP) • Innovative Prosecution Solutions for Combating Violent Crime and Opioid Abuse • Justice and Mental Health Collaboration Program (JMHCP) • Helping Children and Youth Impacted by Opioids • Opioid Affected Youth Initiative • Mentoring Strategies for Youth Impacted by Opioids • Adult Drug Court Discretionary Grant Program • Veterans Treatment Courts • Drug Treatments Courts Program • Opioid-Related Research for Criminal Justice Purposes • Paul Coverdell Forensic Science Improvement Grant Program National Institute on Drug Abuse (NIDA) • NIH – HEAL Initiative (Helping to End Addiction Long-Term) Administration for Community Living (ACL) • NIDDLR – Brandeis INROADS Project • Traumatic Brain Injury State Partnership Program (TBISPP) State level appropriated dollars List is not exhaustive of all $$ allocated to the Opioid Crisis
Evidence-Based Approaches • Medication Assisted Treatment • Eliminating Prior authorizations • Initiating it in Emergency Departments • Expanding to other settings • Naloxone – Wide Distribution • Academic Detailing - (Technical Assistance for Medical providers) • Prescription Drug Monitoring Programs in 49 States • Enhanced Morbidity-Mortality Surveillance in 45 States • Fentanyl screening in Clinical toxicology testing • 911 Good Samaritan Laws • Syringe Service Programs
Opioid Use and Mental Health Concerns Workgroup Traumatic Brain Injury State Partnership Program (TBISPP) 2018-2021 Grant Cycle • Mentor States: Massachusetts and Virginia (participation from Indiana) • Partner States: Kentucky, Maryland and North Carolina “The mission of the ACL - Opioid Use and Mental Health Concerns workgroup is to identify and share best practices across states with regard to addressing the intersections between substance use-related disorders, mental health and brain injuries. This will be accomplished by developing and widely-sharing tools related to that goal.”
Substance Use-Related Disorders (SUD)
Diagnostic and Statistical Manual-V Clinical Criteria: Substance Use Disorder Based on a problematic pattern of use of the substance with clinical significant distress or impairment (at least two symptoms in a 12 month period) • Impaired control • Social impairment • Risky Use • Pharmacological criteria • Determination of severity ACL WORKGROUP FOCUS – Alcohol, Drugs, and Prescription Use and Misuse
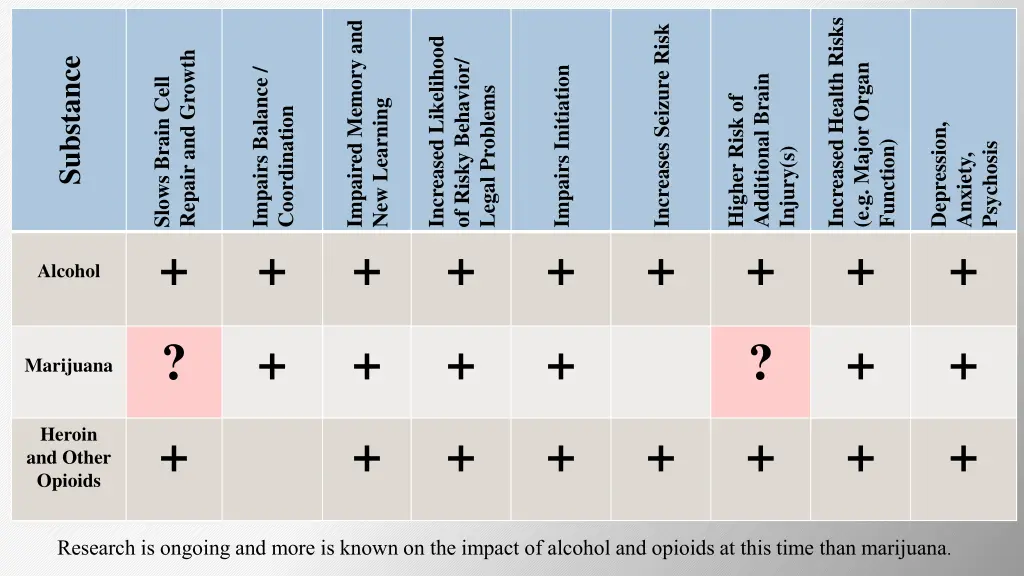
Impaired Memory and + Increased Health Risks Increases Seizure Risk + Increased Likelihood Repair and Growth Substance of Risky Behavior/ + (e.g. Major Organ + Impairs Initiation + Impairs Balance / + Additional Brain + Slows Brain Cell + Legal Problems Higher Risk of New Learning Coordination Depression, Psychosis Function) Injury(s) Anxiety, + Alcohol ? + + + + ? + + Marijuana Heroin and Other Opioids + + + + + + + + Research is ongoing and more is known on the impact of alcohol and opioids at this time than marijuana.
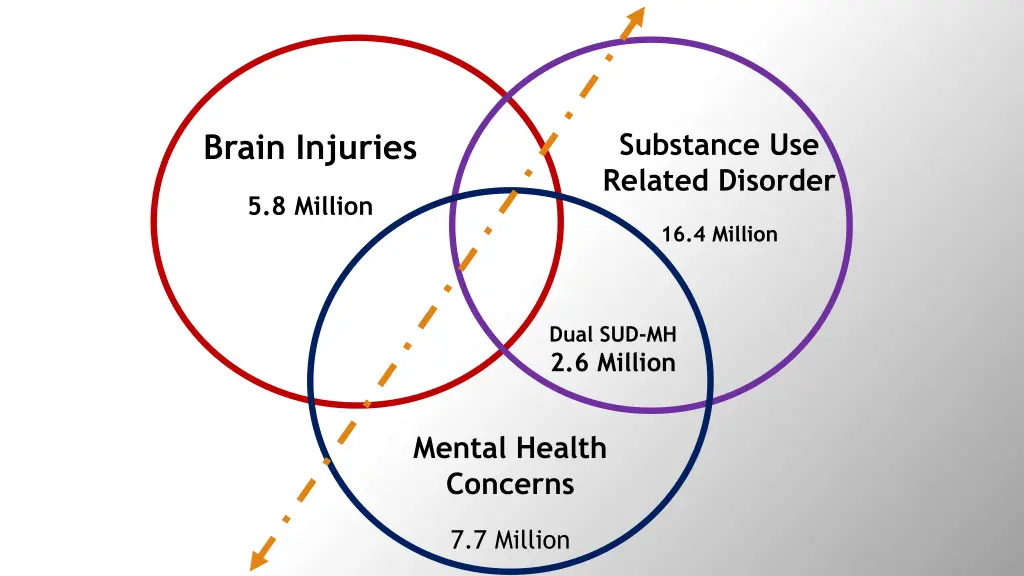
Substance Use Related Disorder Brain Injuries 5.8 Million 16.4 Million Dual SUD-MH 2.6 Million Mental Health Concerns 7.7 Million
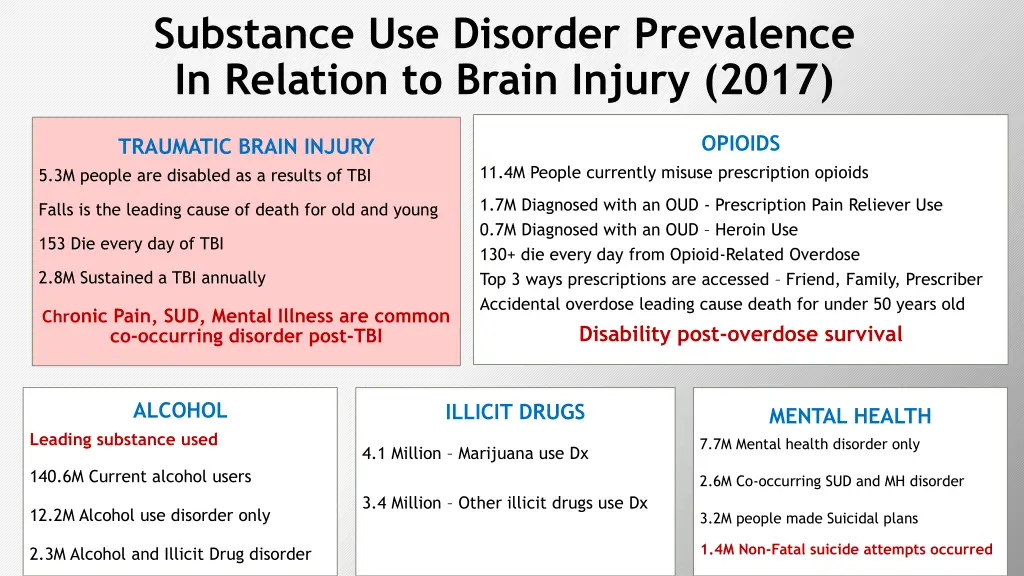
Substance Use Disorder Prevalence In Relation to Brain Injury (2017) OPIOIDS TRAUMATIC BRAIN INJURY 5.3M people are disabled as a results of TBI 11.4M People currently misuse prescription opioids 1.7M Diagnosed with an OUD - Prescription Pain Reliever Use 0.7M Diagnosed with an OUD – Heroin Use 130+ die every day from Opioid-Related Overdose Top 3 ways prescriptions are accessed – Friend, Family, Prescriber Accidental overdose leading cause death for under 50 years old Disability post-overdose survival Falls is the leading cause of death for old and young 153 Die every day of TBI 2.8M Sustained a TBI annually Chronic Pain, SUD, Mental Illness are common co-occurring disorder post-TBI ALCOHOL ILLICIT DRUGS MENTAL HEALTH 7.7M Mental health disorder only Leading substance used 4.1 Million – Marijuana use Dx 140.6M Current alcohol users 2.6M Co-occurring SUD and MH disorder 3.4 Million – Other illicit drugs use Dx 12.2M Alcohol use disorder only 3.2M people made Suicidal plans 1.4M Non-Fatal suicide attempts occurred 2.3M Alcohol and Illicit Drug disorder
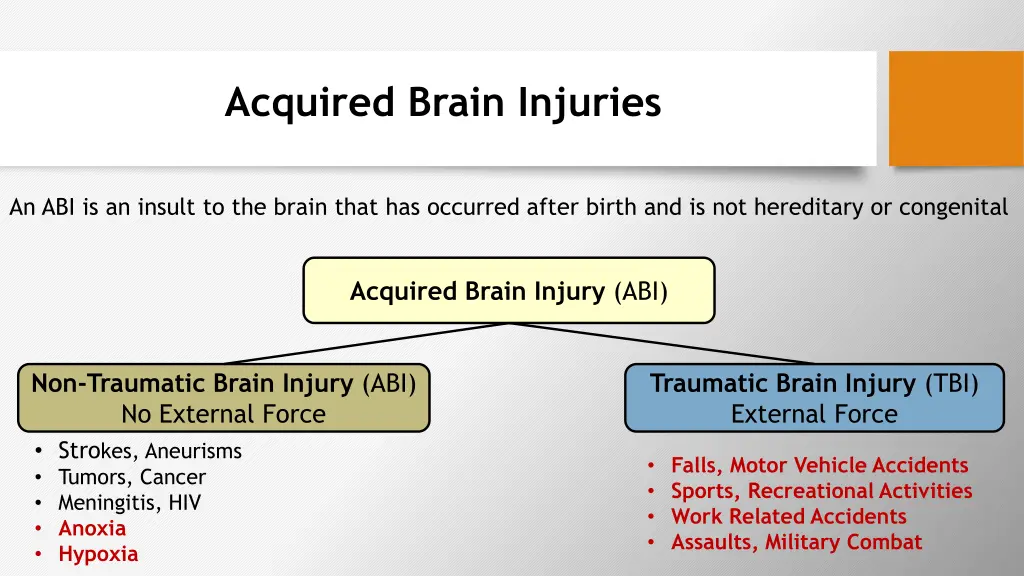
Acquired Brain Injuries An ABI is an insult to the brain that has occurred after birth and is not hereditary or congenital Acquired Brain Injury (ABI) Non-Traumatic Brain Injury (ABI) No External Force • Strokes, Aneurisms • Tumors, Cancer • Meningitis, HIV • Anoxia • Hypoxia Traumatic Brain Injury (TBI) External Force • Falls, Motor Vehicle Accidents • Sports, Recreational Activities • Work Related Accidents • Assaults, Military Combat
Non-Fatal Overdoses Overdose event where the person is revived • Naloxone Suppressed breathing and heart rate • Shallow breaths OR Not breathing • Loss of consciousness may occur Time sensitive emergency • 3-6 minutes irreversible brain damage Overdose survivors can sustain various injuries • Hypoxic Injury – NOT ENOUGH oxygen flow to the brain • Anoxic injury – NO oxygen flow to the brain • TBI – Increase risk of Fall during overdose event
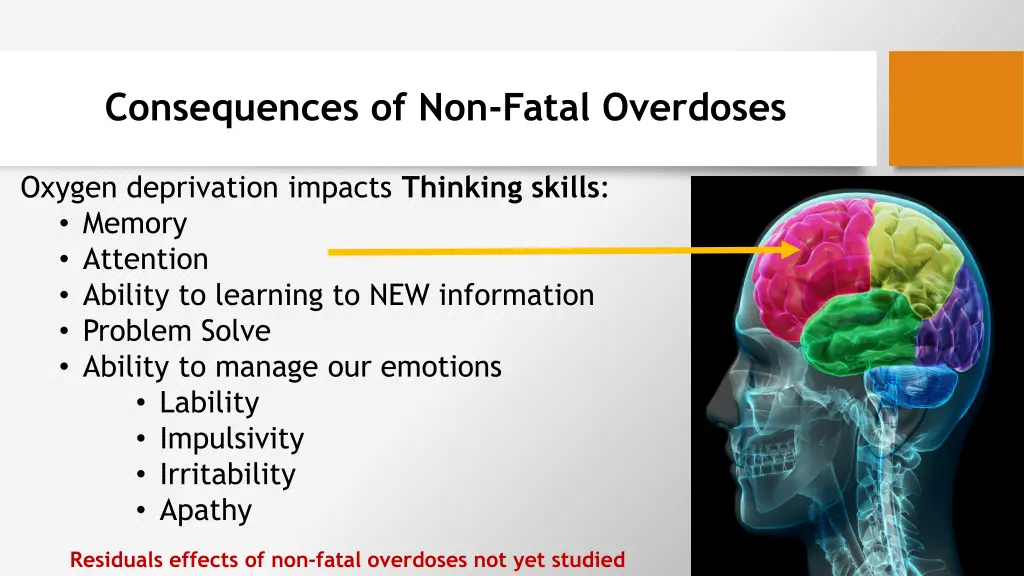
Consequences of Non-Fatal Overdoses Oxygen deprivation impacts Thinking skills: • Memory • Attention • Ability to learning to NEW information • Problem Solve • Ability to manage our emotions • Lability • Impulsivity • Irritability • Apathy Residuals effects of non-fatal overdoses not yet studied
Acquired Brain Injuries Continued… Brain Injury can result in a chronic disability that may • Worsen with age • Complicate pre-existing/co-morbid condition(s) • Increase risk of sustaining additional brain injuries • Further decline functioning with every SUBSEQUENT injury
Intersections: SUD and Brain Injuries
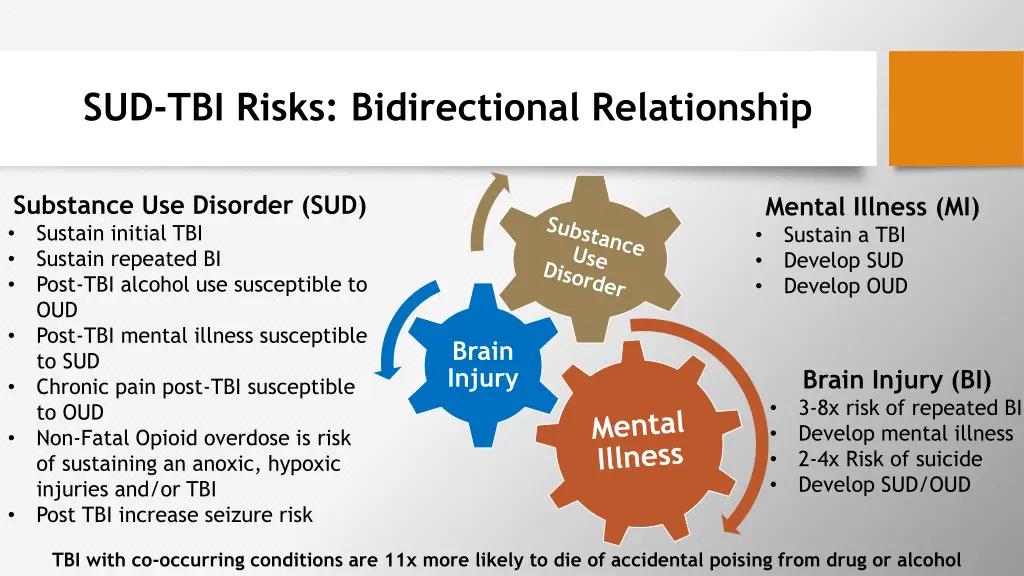
SUD-TBI Risks: Bidirectional Relationship Substance Use Disorder (SUD) • Sustain initial TBI • Sustain repeated BI • Post-TBI alcohol use susceptible to OUD • Post-TBI mental illness susceptible to SUD • Chronic pain post-TBI susceptible to OUD • Non-Fatal Opioid overdose is risk of sustaining an anoxic, hypoxic injuries and/or TBI • Post TBI increase seizure risk Mental Illness (MI) Sustain a TBI Develop SUD Develop OUD • • • Brain Injury Brain Injury (BI) 3-8x risk of repeated BI Develop mental illness 2-4x Risk of suicide Develop SUD/OUD • • • • TBI with co-occurring conditions are 11x more likely to die of accidental poising from drug or alcohol
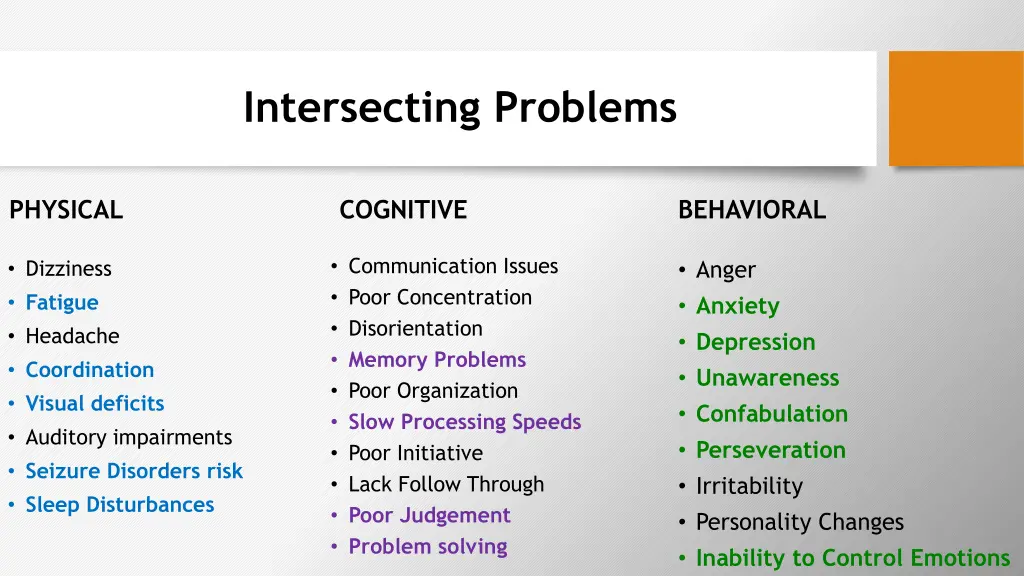
Intersecting Problems PHYSICAL COGNITIVE BEHAVIORAL • Communication Issues • Poor Concentration • Disorientation • Memory Problems • Poor Organization • Slow Processing Speeds • Poor Initiative • Lack Follow Through • Poor Judgement • Problem solving • Anger • Anxiety • Depression • Unawareness • Confabulation • Perseveration • Irritability • Personality Changes • Inability to Control Emotions • Dizziness • Fatigue • Headache • Coordination • Visual deficits • Auditory impairments • Seizure Disorders risk • Sleep Disturbances
Challenges to Engagement Resulting from TBI Families & Caregiver • Can feel trapped, isolated, abandoned • Can become be targets of abuse by survivor • Can be annoyed and impatient with survivor Service Providers • May end services pre-maturely if survivors are viewed (labeled) as resistant, aggressive, disinterested, not motivated, lazy, or non-compliant. • Survivors can overtime burn bridges with service providers • Patience, accommodating symptoms of TBI and connecting to brain injury services can help
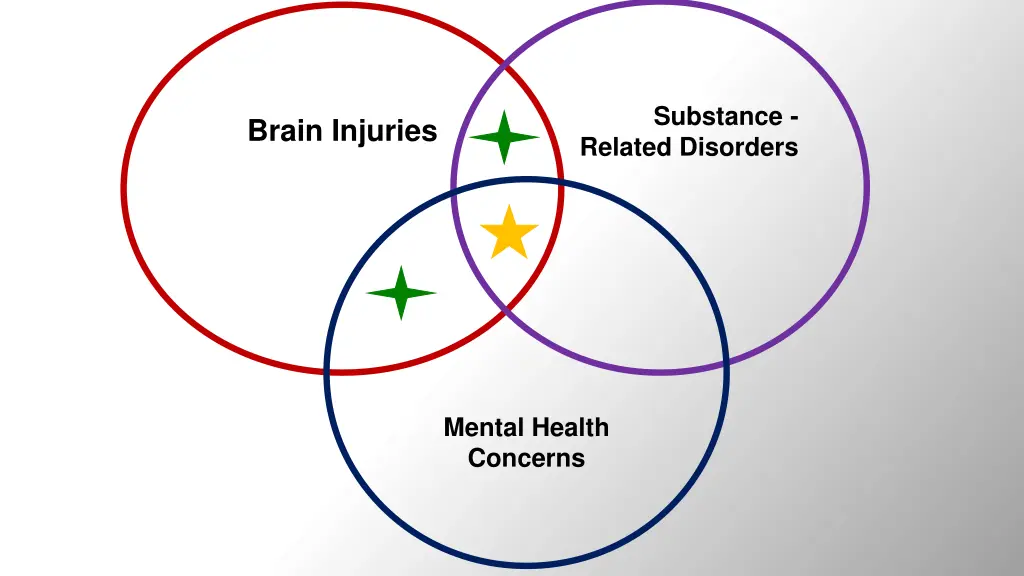
Substance - Brain Injuries Related Disorders Mental Health Concerns
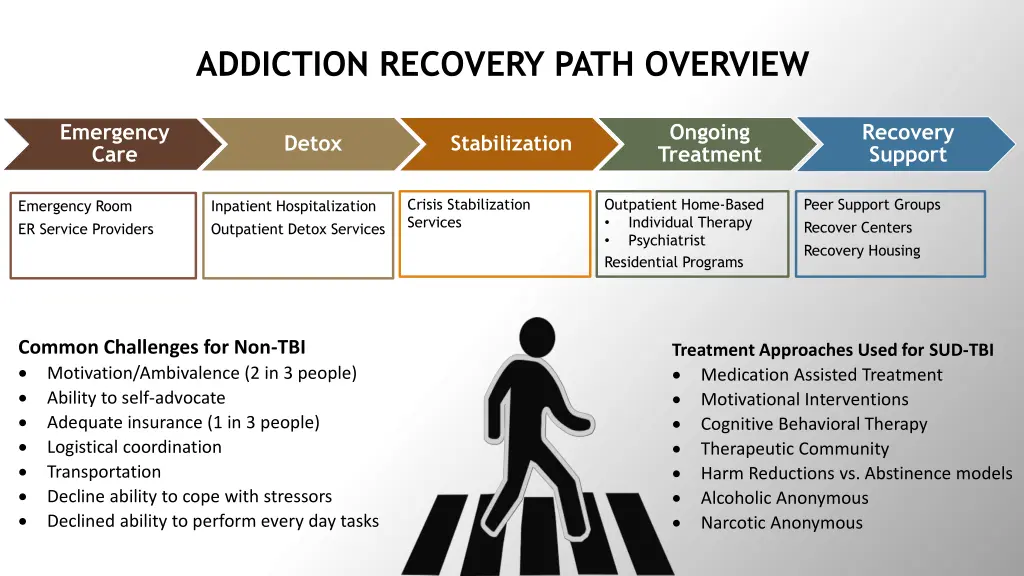
ADDICTION RECOVERY PATH OVERVIEW Emergency Care Ongoing Treatment Recovery Support Detox Stabilization Crisis Stabilization Services Outpatient Home-Based • Individual Therapy • Psychiatrist Residential Programs Peer Support Groups Recover Centers Recovery Housing Emergency Room ER Service Providers Inpatient Hospitalization Outpatient Detox Services Common Challenges for Non-TBI Motivation/Ambivalence (2 in 3 people) Ability to self-advocate Adequate insurance (1 in 3 people) Logistical coordination Transportation Decline ability to cope with stressors Declined ability to perform every day tasks Treatment Approaches Used for SUD-TBI Medication Assisted Treatment Motivational Interventions Cognitive Behavioral Therapy Therapeutic Community Harm Reductions vs. Abstinence models Alcoholic Anonymous Narcotic Anonymous
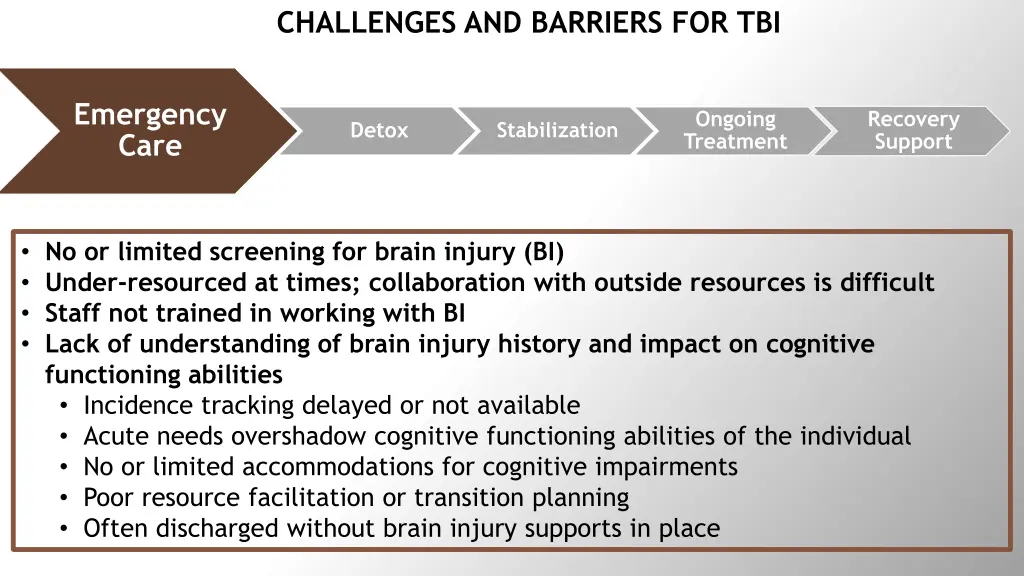
CHALLENGES AND BARRIERS FOR TBI Emergency Care Ongoing Treatment Recovery Support Detox Stabilization • No or limited screening for brain injury (BI) • Under-resourced at times; collaboration with outside resources is difficult • Staff not trained in working with BI • Lack of understanding of brain injury history and impact on cognitive functioning abilities • Incidence tracking delayed or not available • Acute needs overshadow cognitive functioning abilities of the individual • No or limited accommodations for cognitive impairments • Poor resource facilitation or transition planning • Often discharged without brain injury supports in place
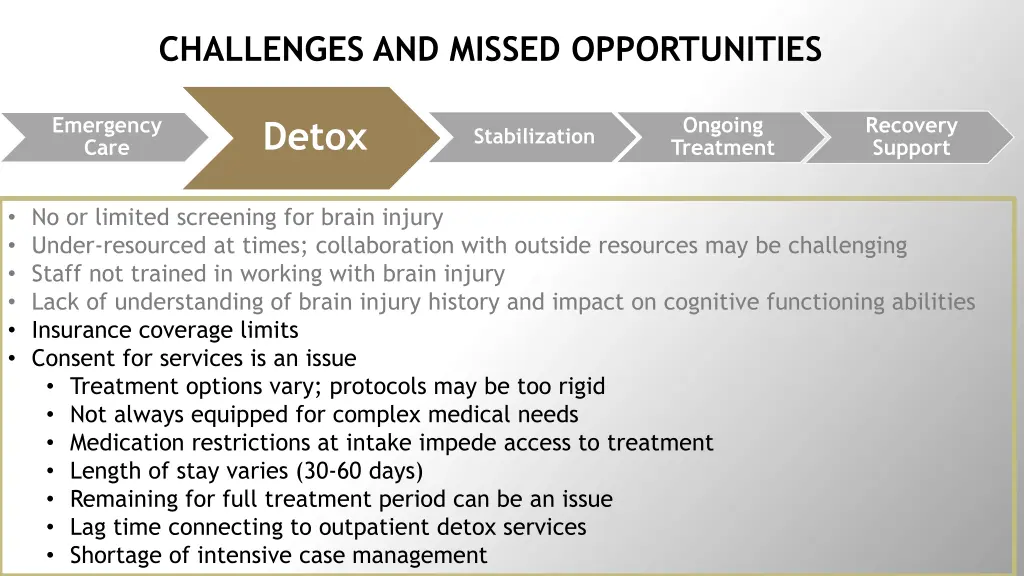
CHALLENGES AND MISSED OPPORTUNITIES Emergency Care Ongoing Treatment Recovery Support Detox Stabilization • No or limited screening for brain injury • Under-resourced at times; collaboration with outside resources may be challenging • Staff not trained in working with brain injury • Lack of understanding of brain injury history and impact on cognitive functioning abilities • Insurance coverage limits • Consent for services is an issue • Treatment options vary; protocols may be too rigid • Not always equipped for complex medical needs • Medication restrictions at intake impede access to treatment • Length of stay varies (30-60 days) • Remaining for full treatment period can be an issue • Lag time connecting to outpatient detox services • Shortage of intensive case management
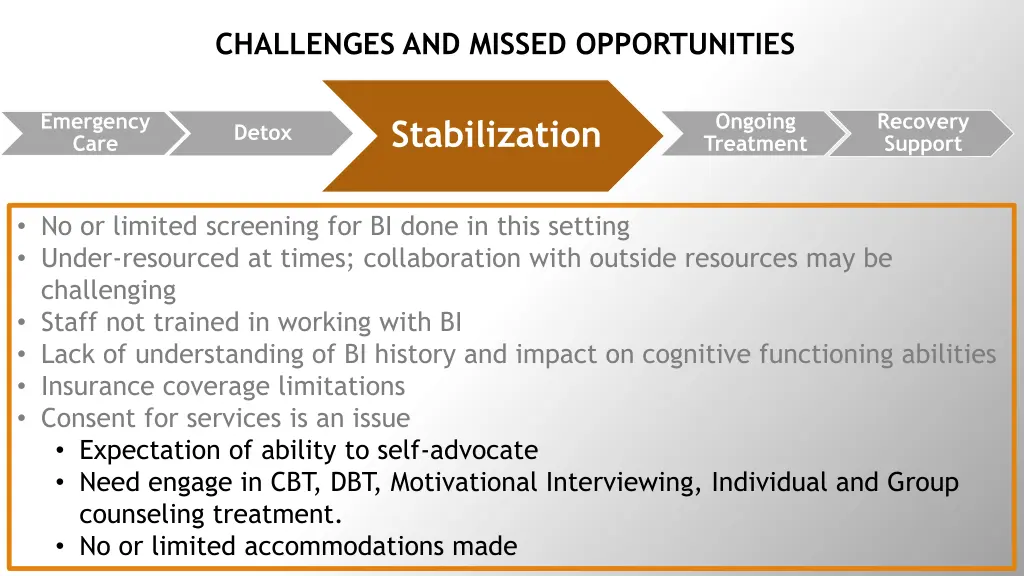
CHALLENGES AND MISSED OPPORTUNITIES Emergency Care Ongoing Treatment Recovery Support Stabilization Detox • No or limited screening for BI done in this setting • Under-resourced at times; collaboration with outside resources may be challenging • Staff not trained in working with BI • Lack of understanding of BI history and impact on cognitive functioning abilities • Insurance coverage limitations • Consent for services is an issue • Expectation of ability to self-advocate • Need engage in CBT, DBT, Motivational Interviewing, Individual and Group counseling treatment. • No or limited accommodations made
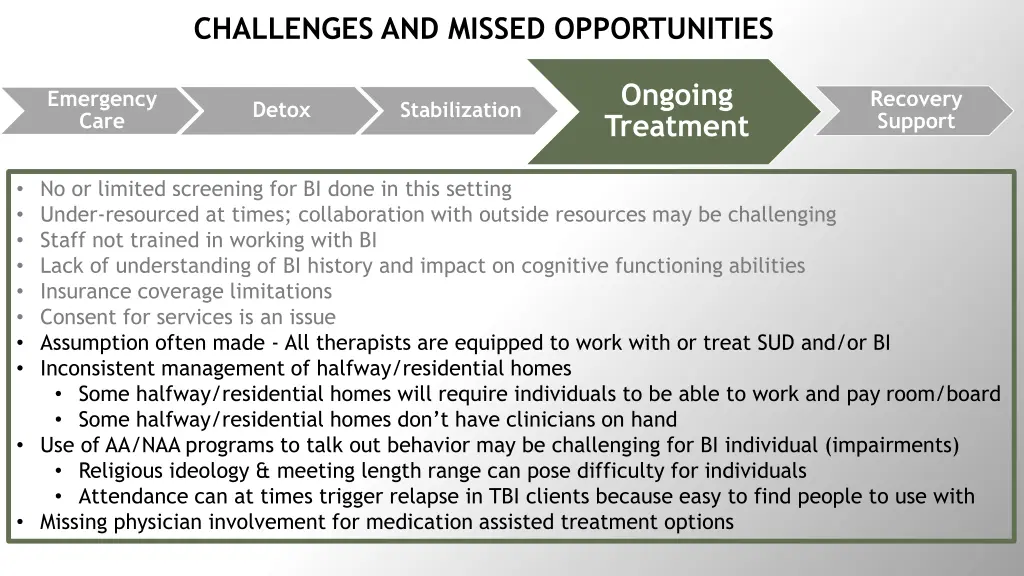
CHALLENGES AND MISSED OPPORTUNITIES Ongoing Treatment Emergency Care Recovery Support Detox Stabilization • No or limited screening for BI done in this setting • Under-resourced at times; collaboration with outside resources may be challenging • Staff not trained in working with BI • Lack of understanding of BI history and impact on cognitive functioning abilities • Insurance coverage limitations • Consent for services is an issue • Assumption often made - All therapists are equipped to work with or treat SUD and/or BI • Inconsistent management of halfway/residential homes • Some halfway/residential homes will require individuals to be able to work and pay room/board • Some halfway/residential homes don’t have clinicians on hand • Use of AA/NAA programs to talk out behavior may be challenging for BI individual (impairments) • Religious ideology & meeting length range can pose difficulty for individuals • Attendance can at times trigger relapse in TBI clients because easy to find people to use with • Missing physician involvement for medication assisted treatment options
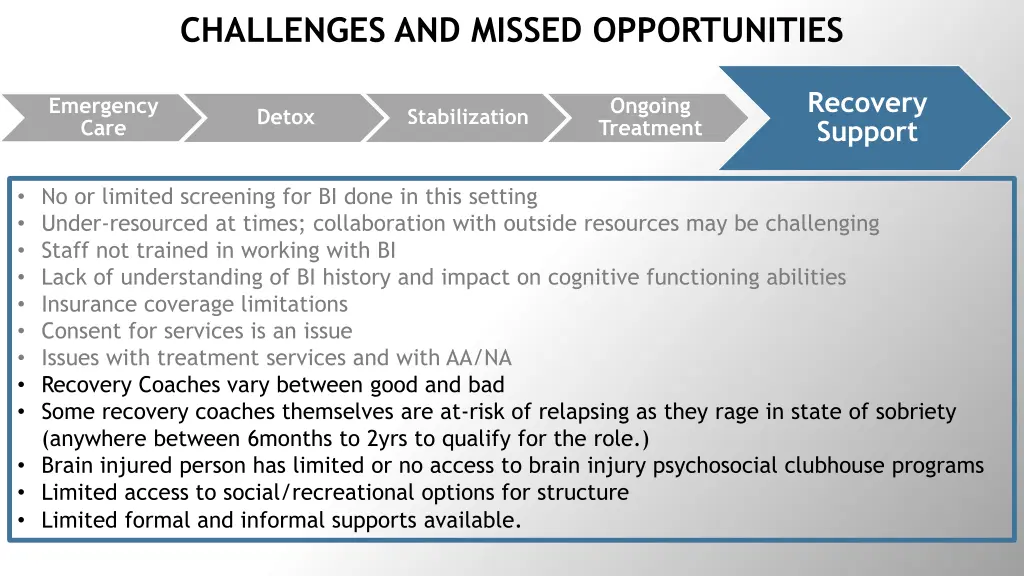
CHALLENGES AND MISSED OPPORTUNITIES Recovery Support Emergency Care Ongoing Treatment Detox Stabilization • No or limited screening for BI done in this setting • Under-resourced at times; collaboration with outside resources may be challenging • Staff not trained in working with BI • Lack of understanding of BI history and impact on cognitive functioning abilities • Insurance coverage limitations • Consent for services is an issue • Issues with treatment services and with AA/NA • Recovery Coaches vary between good and bad • Some recovery coaches themselves are at-risk of relapsing as they rage in state of sobriety (anywhere between 6months to 2yrs to qualify for the role.) • Brain injured person has limited or no access to brain injury psychosocial clubhouse programs • Limited access to social/recreational options for structure • Limited formal and informal supports available.

Kentucky’s Cabinet for Health and Family Service – Department of Aging and Independent Living Partnerships: Department of Behavioral Health Activities: • Develop sustainable relationship • Identify magnitude of the problem • BI Screening • Technical Assistance Community Mental Health Centers Psychiatric Centers Outpatient Treatment Centers Target: • Providers County Jails

Massachusetts Rehabilitation Commission Partnerships: Activities: • SUD-TBI Train-the-Trainer Model • Screening for BI and SUD MA Department of Public Health • Intensive Case Management Pilot Executive Office of Elder Affairs • Technical Assistance • MRC SUD Task Force Target: MassHealth • SUD/OUD Providers, Brain injury Providers Brain Injury Association of MA • Aging agencies and Independent living centers staff • Hospital and Nursing facility Staff BAMSI – New Start Head Injury Center • Community Health Centers • Recovery Coaches and Peer mentors • MassHealth navigators • Home Care providers, Day programs
Maryland Behavioral Health Administration Partnerships: Activities: • Training and Education • BI Screening • Technical Assistance MD Department of Aging MD Department of Disabilities Target: • Behavioral Health professionals • Local Police Department Crisis Intervention Training Coordinator • Overdose Fatality Review Teams MD Developmental Disability Administration MD Crisis Intervention
North Carolina Department of Health and Human Services Activities: • Training and education • TBI screening • Surveillance – BRFSS • Prison system pilot • Technical Assistance Partnerships: SUD Section in the Department Brain Injury Association of NC Managed Care Organizations 1115 Waiver Target: • Community Based providers • SUD Providers SUD providers Prison System (future goal)
Virginia Department of Aging and Rehabilitation Services Partnerships: Activities: • Training and education • BI Screening • Technical Assistance Virginia Alliance of Brain Injury Service Providers Brain Injury Alliance of Virginia VA Department for Behavioral Health and Developmental Disabilities and Local Community Services Boards Target: • Crisis Intervention Service providers • 2 Area Aging Agencies • 2 Free Charitable Clinics • 2 Independent Living Center • 2 Community Service Boards Executive Leadership Team on Opioids and Addiction Virginia Department of Health, Emergency Medical Service Advisory Board National Alliance on Mental Illness, Virginia Chapter University of Virginia
West Virginia University Center for Excellence in Disabilities in TBI Services Program Activities: • Hosting this forum to talk about SUD-TBI • Expansion of TBI screening in additional populations • Technical assistance and resource coordination to individual with TBI • Exploring the expansion of the TBI definition to include additional causes of anoxia • WVDHHR Bureau for Medical Services implementation of a statewide SUD Waiver Potential Partnerships: WVDHHR Bureau for Medical Services Local health organizations Community support organizations Great River Regional Systems for Addiction/Project Hope (Marshall Health) Recovery Point Target: • Providers • People living with brain injuries Mental health agencies
Take Away • Gather data on TBI –SUD sub-populations. • Expand Brain Injury services to include secondary injury due to opioid overdose(s) • Establish cross systems partnerships • Improve resource facilitation across intervention settings and community based providers • Develop or expand on a Day program/Club House Model • Find more ways to support families and caregivers
West Virginia Center for Excellence in Disabilities http://cedwvu.org/ http://cedwvu.org/resources/ RESOURCE
Contact Information Gabriela Lawrence-Soto, ACL Grant Project Manager, Massachusetts Rehabilitation Commission Gabriela.Lawrence-soto@massmail.state.ma.us • Donna Cantrell, Med – ACL Grant Program Specialist, Brain Injury Services Coordinator, Virginia Department for Aging & Rehabilitative Services donna.cantrell@dars.virginia.gov • Tonia Wells - Director of Brain Injury Services, ACL Project Director, Kentucky Cabinet for Health and Family Services, Department of Aging and Independent Living. ToniaA.Wells@ky.gov • Anastasia B. Edmonston MS CRC,- ACL Grant Program Coordinator, Maryland Behavioral Health Administration anastasia.edmonston@maryland.gov • Scott Pokorny, MSW, CBIS, Traumatic Brain Injury Team Lead, Division of Mental Health, Developmental Disabilities and Substance Abuse Services Scott.Pokorny@dhhs.nc.gov •

References Adams R. S and Corrigan J., “The Intersection of lifetime history of Traumatic Brain Injury and Opioid Epidemic”. October 2018. Addictive Behaviors. Volume 90, Pages 143-145. https://www.sciencedirect.com/science/article/abs/pii/S0306460318310098?via%3Dihub Anastasia Edmonston, Laura Bartolomei-Hill and Jasmine McLendon Presentation – “The Intersection of Opioids and Brain Injury: Addressing Addiction Through a Brain Injury Informed Lens” (2018) https://bha.health.maryland.gov/Documents/The%20Intersection%20of%20Opioids%20and%20Brain%20Injury- %20Addressing%20Addiction%20Through%20a%20Brain%20Injury%20Informed%20Lens.pdf A State without Stigma Campaign. https://www.mass.gov/state-without-stigma A State without Stigma: What is Stigma? - https://www.mass.gov/service-details/what-is-stigma ACL – Traumatic Brain Injury State Partnership Program - https://acl.gov/programs/post-injury-support/traumatic-brain-injury-tbi Bombardier et al, 2010 Brain Injury Association of America. “Non-lethal Opioid Overdose & Acquired Brain Injury”. https://www.biausa.org/public-affairs/media/non-lethal- opioid-overdose-acquired-brain-injury Brain Injury Association of America. “Opioid Overdose Increase Continues Nationwide”. March 6, 2018. https://www.biausa.org/public-affairs/public- awareness/news/opioid-overdose-increase-continues-nationwide Brain Injury Association of VA. “Opioid and Brain Injury” Quick Guide. https://www.biav.net/opioids-brain-injury/ Brain Line - Traumatic Brain Injury Basics - https://www.brainline.org/tbi-basics/what-tbi CDC – Drug Overdose Resources - https://www.cdc.gov/drugoverdose/resources/graphics.html CDC – Evidence-Based Strategies - https://www.cdc.gov/drugoverdose/pdf/pubs/2018-evidence-based-strategies.pdf CDC – Overdose Basics, https://www.cdc.gov/drugoverdose/opioids/ CDC - Overview of the Drug Overdose Epidemic: Behind the Numbers https://www.cdc.gov/drugoverdose/data/index.html • • • • • • • • • • • • • •
References CDC – Resources - https://www.cdc.gov/drugoverdose/resources/graphics.html CDC – Severe Traumatic Brain Injury https://www.cdc.gov/traumaticbraininjury/severe.html CDC – TBI and Statistics - https://www.cdc.gov/traumaticbraininjury/data/index.html CDC – TBI: Get the Facts. https://www.cdc.gov/traumaticbraininjury/get_the_facts.html CDC – Traumatic Brain Injury and Concussion Publications, Reports, and Fact Sheets. www.cdc.gov/traumaticbraininjury/pubs/index.html CDC – Understanding the Epidemic - www.cdc.gov/drugoverdose/epidemic/index.html Corrigan and Mysiw in “Substance Abuse Among Person’s with Traumatic Brain Injury” Brain Injury Medicine, 2nd Edition 2012 Drug Abuse.com "Symptoms and signs of Drug Abuse". https://drugabuse.com/symptoms-signs-drug-abuse-effects/ Harrison-Felix C., Pretz C., Hammond, FM., Cuthbert, JP., Corrigan, J., miller, AC., Haarbauer-Krupa, J. (2014) Life Expectancy after Inpatient Rehabilitation for Traumatic Brain Injury in the United States. J. Neurotrauma.31:1-9. HHS - "U.S Department of Health and Human Services Awards Over 1 Billion to Combat Opioid Crisis". September 2018 - https://www.hhs.gov/about/news/2018/09/19/hhs-awards-over-1-billion-combat-opioid-crisis.html HHS - “Strategy to Combat Opioid Abuse, Misuse, and Overdose: A Framework Based on the Five Point Strategy” report by U.S. Department of Health and Human Services, 2017. https://www.hhs.gov/opioids/sites/default/files/2018-09/opioid-fivepoint-strategy-20180917-508compliant.pdf HHS - U.S. Department of Health Human Services - Opioids (January 2019). http:///www.hhs.gov/opioids/ https://www.drugabuse.gov/drugs-abuse/commonly-abused-drugs-charts John Corrigan, Ph.D., plenary presentation, National Association of State Head Injury Administrators State of the State conference, Des Moines Iowa, 9.25.18 • • • • • • • • • • • • • •
References Massachusetts Department of Public Health – BSAS https://www.mass.gov/orgs/bureau-of-substance-addiction-services Massachusetts Rehabilitation Commission – 2017-2018 Focus Group Results on Barriers to SUD Service for TBI Massachusetts Rehabilitation Commission – Substance Use Disorder (SUD) Summary Survey Report. March 2018. Massachusetts Responds to the Opioid Epidemic - https://www.mass.gov/massachusetts-responds-to-the-opioid-epidemic Massachusetts TBI in Elder Web Course, Modules 1, 4 and 5 - https://elderswebcourse.org/ Model Systems Knowledge Translation Center - https://msktc.org/tbi National Database: 2017 Profile of People with the Traumatic Brain Injury Model Systems. https://msktc.org/lib/docs/Data_Sheets_/2017_TBIMS_National_Database_Update_1.pdf National Public Radio Inc. (NPR) – “What Doesn't Kill You Can Maim: Unexpected Injuries From Opioids” by Martha Bebinger. April 13, 2017. https://www.npr.org/sections/health-shots/2017/04/13/523452905/what-doesnt-kill-you-can-maim-unexpected-injuries-from-opioids New York Time - “Short Answers to Hard Questions, About the Opioid Crisis” Article by Josh Katz UPDATED August 10, 2017. www.nytimes.com/interactive/2017/08/03/upshot/opioid-drug-overdose-epidemic.html?wpisrc=nl_health202&wpmm=1 NIDA – Funding Opportunities in Response to Opioid Crisis - https://www.drugabuse.gov/about-nida/noras-blog/2018/12/new-funding-opportunities-in- response-to-opioid-crisis NIDILRR - National Institute on Disability, Independent Living and Rehabilitation Research - https://acl.gov/about-acl/about-national-institute-disability- independent-living-and-rehabilitation-research NIH - Making strides in Helping to End Addiction Long-term (HEAL) - https://www.nih.gov/about-nih/who-we-are/nih-director/statements/making-strides- helping-end-addiction-long-term-heal NIH - National Institute on Drug Abuse - Opioids Brief Summary https://www.drugabuse.gov/drugs-abuse/opioids#summary-of-the-issue Prescription Drug Monitoring Programs - http://www.pdmpassist.org/content/prescription-drug-monitoring-frequently-asked-questions-faq • • • • • • • • • • • • • •
References SAMHSA - "ADVISORY News for the Treatment Field: Treating Clients With Traumatic Brain Injury". October 2010 Volume 9 Issue 2, https://store.samhsa.gov/system/files/sma10- 4591.pdf • SAMHSA – Alcohol, Tobacco and other Drugs. https://www.samhsa.gov/find-help/atod • SAMHSA – Common Comorbidities - https://www.samhsa.gov/medication-assisted-treatment/treatment/common-comorbidities • SAMHSA – Grant Programs - https://www.samhsa.gov/programs-campaigns/medication-assisted-treatment/training-materials-resources/state-grant-programs • SAMHSA - Key Substance Use and Mental Health Indicators in the United States: Results from the 2017 National Survey on Drug Use and Health. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHFFR2017/NSDUHFFR2017.pdf • SAMHSA – Medication Assisted Treatment - POAD Fact Sheet - https://www.samhsa.gov/sites/default/files/programs_campaigns/medication_assisted/mat-pdoa-fact-sheet.pdf • SAMHSA – Mental Health and Substance Use Disorders - https://www.samhsa.gov/find-help/disorders • SAMHSA - Rx Pain Medications, Know the Options: Get The Facts. https://store.samhsa.gov/system/files/sma17-5053-7.pdf • SAMHSA - SAMHSA’s Efforts to Fight Prescription Drug Misuse and Abuse. https://www.samhsa.gov/prescription-drug-misuse-abuse/samhsas-efforts • Substance Abuse and Traumatic Brain Injury - https://www.brainline.org/article/substance-abuse-and-traumatic-brain-injury • Summary of Responses to RFO: People with Disabilities and Opioid Use Disorder, National Institute on Disability, Independent Living, and Rehabilitation Research retrieved on 8.1.18 https://www.acl.gov/sites/default/files/news%202018-05/20180502NIDILRROpioidRFIFindings.pdf • The Atlantic. “Are Opioids Behind a Cluster of Unusual Amnesia Cases?” By Sarah Zhang. January 30, 2017. https://www.theatlantic.com/health/archive/2017/01/opioids- amnesia/514697/ • Tonic.Vice.com Article – “When an Overdose Doesn’t Kill You” by Jason Silverstein. July 3, 2017. https://tonic.vice.com/en_us/article/ywzd9k/when-an-overdose-doesnt-kill-you • U.S. News. “Memory Loss Hitting Some Fentanyl Abusers” by Dennis Thompson, Health Day Reporter. Jan. 29, 2018. https://health.usnews.com/health-care/articles/2018-01- 29/memory-loss-hitting-some-fentanyl-abusers •