Download
1 / 38
400 likes | 720 Views
This case study follows a 21-year-old male presenting with headache, vision loss, and systemic symptoms, diagnosed with VKH disease. Learn about the diagnostic process, clinical stages, criteria, and treatment outcomes of this autoimmune condition. Discover the importance of early intervention in preventing chronic progression.

E N D
Vogt Koyanagi-Harada Luca Cimino Ambulatorio di Immunologia Oculare Arcispedale S.Maria Nuova Reggio Emilia, Italy Luca Cappuccini Arcispedale S.Maria Nuova Reggio Emilia, Italy
K.A. 21 YEAR OLD M • January 2004: headache, flu-like illness, vertigo. • He thought about his work (welder). • He followed therapy with non steroidal drugs.
K.A. 21 YEAR OLD M • Unfortunately 5 days later his vision decreased and • He went to Ophthalmic Emergency Service of a city University near our Hospital ( was a holiday!). • The patient was visited and because of his history (headache before visual loss) Brain NMR was performed (also because he showed bilateral swelling optic disc).
K.A. 21 YEAR OLD M • But brain NRM was negative for tumor and/or multiple sclerosis signs and/or CNS vasculitis. • Natural VA was 0.4 in both eyes ( 0.6 with -2 sf in RE and 0.7 with -1.75 sf in LE). • Before of this the patient never used glasses.
K.A. 21 YEAR OLD M Bilateral swelling optic disc
K.A. 21 YEAR OLD M • They decided to perform a generous diagnostic sierologic work-up for uveitis (and everything) with negative results except a positive HLA-B51 (well related also at oral aphthae showed from the pt.).
K.A. 21 YEAR OLD M • For a better evaluation the patients underwent a Fluorangiography (also to have time to think about a possible diagnosis)
K.A. 21 YEAR OLD M • But FAG showed only minimal alterations of RPE (it was substasially negative)
K.A. 21 YEAR OLD M OCT: confirmed Bilateral serous retinal detachment
K.A. 21 YEAR OLD M • What about the clinical diagnosis? • bilateral central serous chorioretinopathy (may be due to stress of saudade: the pt live abrod far of his land). • Primary inflammatory choriocapillaropathy (a flu-like episode before visual loss + myopic eyes). • Abortive form of Behçet (HLA-B51+ oral aphtae).
Bilateral serous retinal detachment
K.A. 21 YEAR OLD M • To resolve this doubts the Ophthalmologist sent the patient to us… • What we do?
K.A. 21 YEAR OLD M • The anterior segment was uninflammed in both the eyes. • VA was 0.6 with -2 sf in RE and 0.7 with -1.75 sf in LE • The fundus examination confirmed the swelling disc + showed a bilateral retinal serous detachment in both the eyes.
What I think 1. Posterior exudative uveitis,bilateral. 2. Neurol. signs (hedache + vertigo ). 3. Cutaneous signs (alopecia). 4. No history of penetrating eye trauma or surgery. 5. Negative brain NRM.
What I think • At this point one examination is crucial to confirm the diagnosis ?
Red free photos: RPE detachmentFAG: minimal alterations of RPE.
K.A. 3 Mar 2004 ICG 1.24 ICG 1.35
ICGA: irregularly shaped hypofluorescent zones at middle and late phases
K.A. 21 YEAR OLD M • A lumbar puncture was performed and 178 cells /μL were noted, 100% were lymphocytes. • the diagnosis was reached within 10 days from the onset of symptoms.
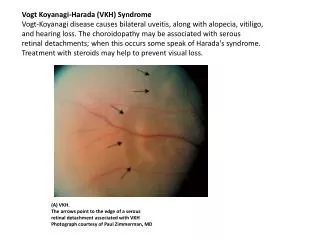
VKH disease: definition • Bilateral granulomatous panuveitis + systemic manifestations. • Unknown etiology. • Auto-immune process against choroidal melanocytes probable.
VKH disease Clinical stages : • Prodromal stage: headache, flu-like illness, vertigo • Ocular exudative phase • Chronic relapsing phase: chronic irido-cyclitis and recurrences 4. Convalescent stage : sunset glow fundus: choroidal depigmentation, RPE alterations, scars of Dalen-Fuchs nodules, cutaneous signs
VKH disease: diagnostic criteria AUS criteria ( despite new criteria in 2001, still very practical) : 1. Iridocyclitis, bilateral 2. Posterior exudative uveitis, bilateral 3. Inflammatory neurol. signs (meningismus, CSF pleiocytosis, tinnitus) 4. Cutaneous signs (vitiligo, alopecia, poliosis) Presence of ¾ criteria = VKH (no prior ocular trauma or surgery)
Therapy • Initial intravenous methylprednisolone 1 g X 3 days, followed by oral prednisone 1.0 mg/kg tapered.
K.A. 21 YEAR OLD M • 31st March ’04: • VA was 1.0 in OU. • Resolution of serous retinal detachment
FAG showed RPE alterations 31st March ’04
ICGA: quasi complete resolution of signs 31st March ’04
K.A. 21 YEAR OLD M • He showed RPE changes • in maculararea. • VA 1.0 in both eyes.
Follow-up • After 2 year the patient showed no recurrenries (VA is full in both eyes). • He showed minimal alterations of RPE. • He followed steroid therapy with 5 mg/die of oral prednisone. • He showed no recurrencies of systemic symptoms (headache and hearing loss).
Conclusion • Early treatment of VKH may prevent its progression into the chronic stage of disease. Goto H., Rao N. : Int Ophthalmol Clin 1990 • The exact time interval from the onset of the symptoms to the initiation of adequate treatment in order to prevent chronic evolution is not known.
Conclusion • The proportion of cases for which early and adequate therapy can prevent chronic evolution is also not known. • Unfortunately, a delay of days, weeks or months cannot be avoided either because of delayed consultation of the patient or delayed diagnosis of the disease because of incomplete clinical picture at onset.