Download
1 / 19
190 likes | 285 Views
A Phase II, Randomized, Placebo-Controlled Study of Once-Weekly Alendronate in HIV-Infected Subjects with Decreased Bone Mineral Density Receiving Calcium and Vitamin D. Grace A McComsey, Michelle A Kendall, Pablo Tebas, Susan Swindells, Evelyn Hogg, Beverly Alston-Smith,

E N D
A Phase II, Randomized, Placebo-Controlled Study of Once-Weekly Alendronate in HIV-Infected Subjects with Decreased Bone Mineral Density Receiving Calcium and Vitamin D Grace A McComsey, Michelle A Kendall, Pablo Tebas, Susan Swindells, Evelyn Hogg, Beverly Alston-Smith, Carol Suckow, Geetha Gopalakrishnan, Constance Benson, and David A Wohl on behalf of the ACTG A5163 team
Background • Decreased bone mineral density (BMD) is prevalent among persons living with HIV infection, as are traditional risk factors for reduced BMD. • Alendronate is a bisphosphonate that inhibits osteoclast-mediated bone resorption and is FDA-approved for the treatment of osteoporosis in men and women. • Small open-label studies of alendronate in combination with calcium and vitamin D in HIV+ individuals suggested the drug increases lumbar spine BMD and is well tolerated (Guaraldi 2004; Mondy 2005; Negredo 2005).
Study Design • A5163 is a 48-week prospective, randomized, double blinded, placebo-controlled trial to evaluate the effects of alendronate versus placebo, with calcium and vitamin D supplementation, on BMD in patients with HIV.
Study Design HIV+ Lumbar t-score ≤-1.5 VL <5000 CD4 > 100 Alendronate + Calcium/Vitamin D n=42 Randomization was stratified by CD4+ cell count at screening (100-200 cells/mm3 or >200 cells/mm3) Placebo+ Calcium/Vitamin D n=40 • Study Regimen: 48 weeks • Alendronate or matching placebo 70 mg weekly • -Calcium carbonate/Vitamin D (500 mg/200IU BID)
Inclusion Documented HIV ≥ 25 years CD4 ≥ 100 cells/mm3 HIV-1 RNA ≤ 5,000 cps/mL Lumbar spine t-score ≤ -1.5 Stable ARV for ≥ 12 wks No plan to alter ARV, exercise habits, or diet Exclusion Pregnancy or breast-feeding Untreated hypogonadism or hyperthyroidism 25-OH vitamin D <15 ng /mL Hepatitis C PTH > 80 pg/mL Chronic systemic steroids Treatment for osteoporosis Recent bone fracture Esophageal pathology Inclusion/Exclusion Criteria
A5163 Main Objectives • To examine the efficacy of once-weekly alendronate and daily calcium and vitamin D in the treatment of HIV-associated decreased BMD, as assessed by percent change in lumbar spine BMD from baseline to week 48 in men receiving alendronate versus placebo • To assess the safety and tolerability of once-weekly alendronate in HIV-infected subjects • To examine gender interactions in the efficacy of once-weekly alendronate and daily calcium and vitamin D in the treatment of HIV-associated decreased BMD
Statistical Considerations • Study powered (80% power; 2-sided alpha = 0.05) to detect an absolute difference of 3.5% in the mean percent change between arms in men. An additional 20% enrolled to account for possible drop-out and unevaluable DXA scans for a total of 27-30 men per arm . • To test for moderate treatment/sex interactions, 10-13 women per arm were also included (total n=80)
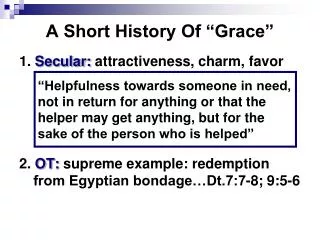
BMD L u m b a r S p i n e (men and women) 5 V i t a m i n D + C a + A l e n d r o n a t e 4 V i t a m i n D + C a * p=0.0003 * p=0.0006 3 % change from baseline † p=0.03 2 * p=0.02 1 0 0 2 4 4 8 * significant within arms † significant between arms W e e k
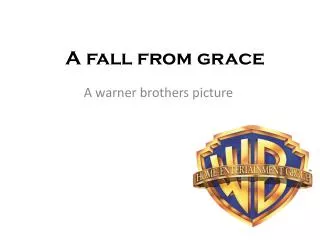
* p<0.0001 * p<0.0001 † p=0.004 † p=0.05 * p=0.03 * p=0.009 * significant within arms † significant between arms
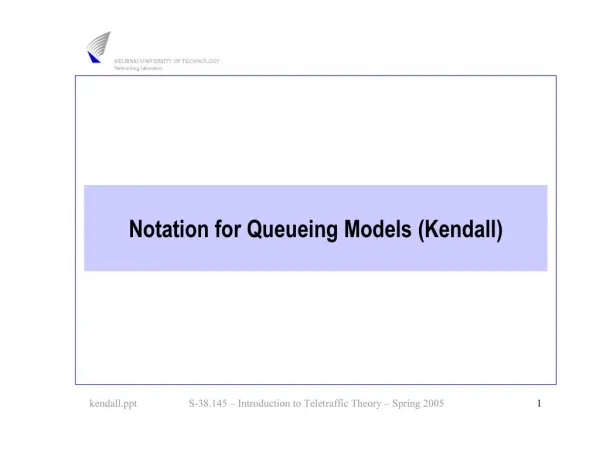
* p=0.0002 * p=0.002 † p=0.007 * significant within arms † significant between arms
Results • Two traumatic fractures occurred during the study (one per arm)
Results • Two traumatic fractures occurred during the study (one per arm). • No evidence of a treatment/sex interaction when we considered the % change from baseline to week 48 in BMD assessed at the lumbar spine, total hip, or trochanter (p=0.41, 0.82, and 0.19, respectively). • Changes from 0 24 weeks strongly predicted changes from 0 48 weeks • In a multivariable model correcting for treatment, BMI and baseline L-spine BMD, black race was associated with a smaller % change from baseline in lumbar spine BMD with alendronate (p=0.003)
Results • Two traumatic fractures occurred during the study (one per arm). • No evidence of a treatment/sex interaction when we considered the % change from baseline to week 48 in BMD assessed at the lumbar spine, total hip, or trochanter (p=0.41, 0.82, and 0.19, respectively). • Changes from 0 24 weeks strongly predicted changes from 0 48 weeks • In a multivariable model correcting for treatment, BMI and baseline L-spine BMD, black race was associated with a smaller % change from baseline in lumbar spine BMD with alendronate (p=0.003)
Results • Two traumatic fractures occurred during the study (one per arm). • No evidence of a treatment/sex interaction when we considered the % change from baseline to week 48 in BMD assessed at the lumbar spine, total hip, or trochanter (p=0.41, 0.82, and 0.19, respectively). • Changes from 0 24 weeks strongly predicted changes from 0 48 weeks • In a multivariable model correcting for treatment, BMI and baseline L-spine BMD, black race was associated with a smaller % change from baseline in lumbar spine BMD with alendronate (p=0.003)
Safety/Tolerability • More signs/symptoms of Grade 3 in the placebo arm (15% versus 0% in the alendronate arm; p=0.01) • No difference between treatment arms in Grade 3 laboratory toxicities (15% on placebo arm versus 17% on alendronate; p>0.9) • No discontinuation related to toxicity
Study Limitations • Osteopenia may not require treatment • Duration relatively short • need longer term efficacy and tolerability • 21% changed ARV during study (5 TDF) • results unchanged when these 5 subjects were excluded
Conclusions • Alendronate given with calcium/vitamin D led to significant increases in lumbar spine, total hip and trochanter BMD • Calcium/vitamin D alone led to modest increases in BMD • Alendronate was well tolerated, without significant adverse events • There was no evidence of treatment/sex interactions at any of the bone sites examined
Acknowledgments • David Wohl • Pablo Tebas • Michelle Kendall • Janet Andersen • Evelyn Hogg • Lynette Purdue • Susan Swindells • Geetha Gopalakrishnan • Melissa G. Kerkau • Marjorie Busby • Carol Suckow • Amy Sbrolla • Enid Vazquez • Jennifer Nowak • Murray Abramson • Anne E. de Papp • Mary E. Melton Merck for alendronate/placebo All Participating ACTU Sites and Study Participants!