SNOMED CT
90 likes | 254 Views
SNOMED CT. Denise Downs Knowledge Management & Education Lead Data Standards, Technology Office Department of Health Informatics Directorate. Why a terminology?. Common vocabulary across the UK required for data communication

SNOMED CT
E N D
Presentation Transcript
SNOMED CT Denise Downs Knowledge Management & Education Lead Data Standards, Technology Office Department of Health Informatics Directorate
Why a terminology? • Common vocabulary across the UK required for data communication • SNOMED CT is the NHS mandated terminology for clinical and data interoperability • Applications such as Summary Care Record, Choose and Book, ePrescribing use SCT for recording clinical data (DM&D part of SCT release) • New messaging requirements such as microbiology requests and results will use SCT • With a common terminology other ‘services’ such as NICE, NHS Evidence, Map of Medicine ... all looking to tag using SCT
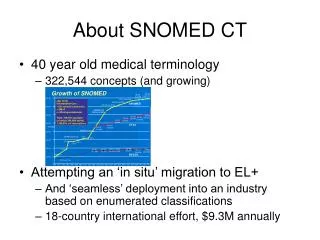
Why SNOMED CT?(SCT) • Current coding systems not scalable, maintainable, or accurately used – and content dated • eg. 587 terms in ICD in relation to accident caused by a pedal cycle • Only something like 3000 terms used in any one year • V12.24 Pedal cyclist injured in collision with two- or three-wheeled motor vehicle, unspecified pedal cyclist, nontraffic accident, while resting, sleeping, eating or engaging in other vital activities • V31.22 Occupant of three-wheeled motor vehicle injured in collision with pedal cycle, person on outside of vehicle, nontraffic accident, while working for income • W65.40 Drowning and submersion while in bath-tub, street and highway, while engaged in sports activity • X35.44 Victim of volcanic eruption, street and highway, while resting, sleeping, eating or engaging in other vital activities
Why SNOMED CT?(cont) • International • 12 countries collaboratively developing and growing • Includes USA, Canada, Australia • Also non English speaking, and being translated • Rich terminology not just list of codes • Provides for more sophisticated searching, reporting, investigation
Optometry and SNOMED CT • There is a large amount of content relevant to Optometry in SCT – needs verifying by Optometry domain experts • Descriptions may need enriching to support optometry – remember SCT is international, concept is unique but can have additional descriptions • May need some new concepts adding – there is a request mechanism
SCT Submission request process • There is a request process for new concepts to be added to SCT • You need to register on the site • It is helpful for these to be well formed requests • https://www.uktcregistration.nss.cfh.nhs.uk/requests/myRequests.jsf
Subsets • SCT contains over 500,000 terms – not all relevant to Optometry • Subsets ‘hold’ concepts within SCT that are relevant to a particular specialism – ie most regular used vocabulary – can be used within software to support pick lists etc on forms • Subsets usually developed by a group; sometimes brought together through a Royal College or Association; to provide an area domain subset used by all suppliers within that domain • Development of Subsets – ideally via ‘rules’ – as SCT is not static
Some considerations: • Patient Identification - and how to make referrals into the NHS, checking medications of own patients if required • What is required ‘outside’ immediate practice as well as within • eg. Accepting referrals, government required statistics, care pathways (diabetes), reporting ....
Next Steps ... • Identify use cases .... what to record, why, what messages needed to go out of system and what will be received • Undertake analysis - requirement for structured data, messages indicates record in SCT, data for re-use is prime candidate for SCT coding - and hence need for SCT usually ‘drops out’ of analysis – free text in systems usually for data not to be re-used • Agree commonality for shared data elements in data model, consult other work such as LRA • Subsets – do as collaboration and share, identify owner and need to keep subset current as new concepts added (why rules help) • Take account of existing research and work – both locally and internationally that can inform eg diabetic retinopathy