Download
1 / 50
500 likes | 596 Views
Explore normal ovary functions, polycystic ovary syndrome, various ovarian tumors, and genetic influences on ovarian cancers. Learn about classification, etiology, histology, and clinical features associated with these conditions.

E N D
Ovary Dr. Amitabha Basu MD
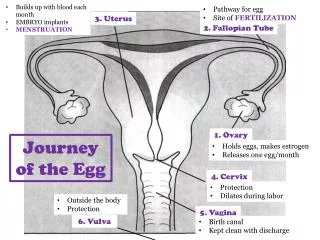
Topic • Normal ovary • Polycystic ovary • Tumors of the ovary
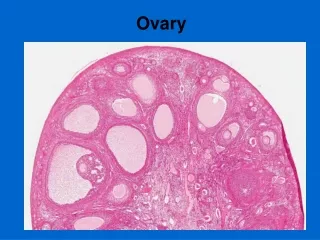
Micro Th) Theca (MG) Membrana granulosa (CR) Corona radiata (ZP) Zona pellucida (CL) Corpus luteum
Polycystic ovarian disease • Definition • Morphology • Clinical features
Pathophysiology • Excessive secretion of estrogen and androgen. • High LH • Low FSH • LH/FSH Ratio: high
Clinical features/complications • Oligomenorrhoea (Polycystic ovarian disease with oligomenorrhea is known as Stein-Leventhal syndrome) • Hirsuitism • Infertility • Endometrial Hyperplasia.
Classification Subtypes Age Incidence Etiopathogenesis Serous tumors Mucinous tumors Dysgerminoma Teratoma Granulosa-theca cell tumor Sertoli Leydig cell tumor Metastasic tumor Tumors of the Ovary
Classification • Tumor arising form the surface epithelium • Tumor arising form the germ cells • Tumor arising form Sex-cord stroma surface epithelium • Metastasic tumor
Multiparty Family history Genes BRCA 1 AND BRCA 2 ( IN HEREDITARY OVARIAN CANCER) ERB B2 K-RAS TP53 Etiopathogenesis
Serous tumor : Types • Benign • Borderline • Malignant Note: All surface epithelial tumors can be divided in these three types
Features of Serous tumor • Common ovarian tumor. • Mostly benign. • Cysts are lined by single Ciliated columnar epithelium. • Cyst contain serous fluid. • Bilateral (25%) • Usually Small.
Microscopy of serus tumor: Cysts are lined by single Ciliated columnar epithelium
Borderline Serous Tumor • Between benign cyst adenomas and malignant cystadenocarcinomas lies the grey zone of "borderline" lesions that are not clearly malignant, but are treated as though they could be.
Malignant serous Tumor : Papillary serous cystadenocarcinomas : note papillary areas.
Microscopy : Papillary process and cellular crowding and Psammoma body (not seen)
Spread of the tumor • These neoplasms characteristically spread by "seeding" along peritoneal surfaces. • Marker for Surface epithelial tumors: CA 125
Features of Mucinous tumor • Not common ( 10%), Large • Cysts are lined by single layer Mucin secreting columnar epithelium. • Cyst contain Mucinous gelatinous fluid: if rupture produce Pseudomyxoma peritonei.
Histology : Multilocular cysts lined by a single layer of benign mucinous columnar epithelium.
Teratoma • Types • Dermoid cyst • Immature malignant Teratoma • Struma Ovarii.
Types • Benign Teratoma ( Mature: usually cystic) • Malignant Teratoma( Immature : usually solid) • Monodermal Teratoma ( carcinoid Tumor, struma ovarii)
Benign Teratoma ( Mature)of ovary • It is also called Dermoid cyst. ( because it contains dermal appendages).
Immature Malignant Teratoma • Mean age : 18 years • Features : bulky, solid • Histology : Tissue containing immature neural tissue with neuroepithelial differentiation.
Dysgerminoma • Etiopathogenesis : Occur with gonadal dygenesis. • Radiosensitive tumor : 80% cure • Unilateral
Granulosa-theca cell tumor • Age : Post menopause but any age • Unilateral • Diagnostic point : Presence of call Exner body in Histology. • Function: Secrete estrogen ; promote endometrial, breast carcinoma.
Sertoli Leydig cell tumor • Age: all age • Unilateral • Point for identification: Gross: Yellow brown, solid. Micro: Pink Sertoli Leydig cells. • Clinical effect: Masculinizing ( defeminizing).
Struma ovarii • In this tumor the Teratoma contain predominantly thyroid tissue.
Metastasic tumor • Age: older age • Primary Tumor: Breast, lung, GIT • Big bilateral mass • Example : Tumor name : Krukenberg tumor
Krukenberg tumor • Primary tumor : Gastric adenocarcinoma • Route of metastasis : Seeding through body cavity. • Bilateral always. • Histology : contain “ signet ring” cells.
Nice to Know this Tumor: Thecoma-fibroma • Any age • Unilateral • Produce Meigs syndrome( ovarian tumor with ascites and Hydrothorax)
Review • Endometriosis ( clinical features) • Endometrial Hyperplasia . Etiology with C/F • Dermoid cyst Gross identification. • Leiomyoma identification and c/f • Carcinoma in situ • Granulosa theca cell tumor.
Review • Metastasic tumors • Ectopic pregnancy • Genes for Ovarian cancers. • Clear cell carcinoma • Vaginitis • Lichen sclerosus • Polycystic ovary • Gonorrhea infection (PID) • Anovulatory cycle : and other Causes of DUB