Download
1 / 70
730 likes | 912 Views
Gain insights into different types of pain (nociceptive, neuropathic, mixed) and the mechanism of pain perception. Explore chronic pain and the gate control theory, along with classifications and physiological processes involved in pain perception.

E N D
UNDERSTANDING OF PAIN“ Nociceptive, Neuropathic & Mixed Pain ” Nur Surya Wirawan Department of Anesthesiology, Intensive Care and Pain Management Faculty of Medicine University of Hasanuddin Makassar
Objective After this lecture, participants are able to understand : Definition of Pain Mechanism of Pain perception Nociceptive Pain Neuropathic Pain Mixed Pain Chronic Pain Take Home Messange
Before Eve was created from Adam's Rib, Adam was put into sleep
Descartes (17th Century) First ideas…. Pain was faithfully transmitted from periphery to brain A pure stimulus response relationship
Progress in understanding pain MELZACK and WALL ‘Gate Control Theory’ 1965-
1965 MELZACK and WALL Introduce Hypothesis of “GATE CONTROL THEORY” Brain GATE CONTROL SYSTEM Aβ - + + DHN ACTION SYSTEM SG - + - C The beginning of “MODULATION”
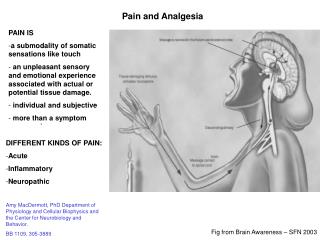
Definition of Pain • Scientific : Pain is unpleasant sensory and emotional experience ascociated with actual or potential tissue damage or describe in term of such damage. (Merskey ,accepted by IASP 1979) • Clinical : “Pain is whatever the experiencing person says. (Mc Caffery 1997) “Pain is what ever the pateint says”
From this definition, some conclusions can be obtained; • PHYSIOLOGICAL PAIN, is a normal sensation, elicited by potential tissue damage Withdrawal reflex • PATHOPHYSIOLOGICAL PAIN, is an abnormal sensation : • Due to actual tissue damage inflamed pain = clinical pain = acute pain e.g. : postoperative pain • Due to nervous system damage neuropathic pain • PATHOLOGICAL PAIN, • Described in intern of such damage CHRONIC PAIN • Chronic pain is now consider as “a disease of entity”. Causing suffering, reducing QOL
KLASIFIKASI NYERI Menurut waktu Nyeri akut & kronik N Y E R I • Menurut patofisiologinya : • Nyeri fisiologik • Nyeri klinis ( nyeri patofisiologik) • Nyeri nosiseptif • Nyeri neuropatik • Perifer • Sentral • 3. Nyeri psikogenik / idiopatik
Acute Pain Acute Pain is the normal predicted physiological response to an adverse chemical, thermal or mechanical stimulus …., associated with surgery, trauma and acute illness.”“ ( Federation of State Medical Boards of US )
Acute pain (Pain of recent onset and probable limited duration, IASP) • Acute onset, localized, sharp and high intensity pain. • Usually self limiting. • Signs of physiologic response of various organs or systems, e.g. sweating, palpitation and increased of blood pressure. • Identifiable causes or related to injury or diseases
Causes of acute pain • Trauma • Surgery • Delivery • Invasive medical procedures • Acute illness.
Acute Pain • constant • sharp aching • well localized Somatic pain Visceral pain • constant • dull aching • poorly localized • usually with nausea and vomit • occasional colicky or cramp • often referred to cutaneous sites
Referred Pain Figure 10-13: Referred pain
There are two sensory afferent neurons • Large myelinated A fibers, very fast conduction velocity. Respond to innocuous stimuli • Small myelinated A & C unmyelinated fibers, have slow conduction velocity. Respond to noxious stimuli Large fibers A Dorsal root ganglion Dorsal Horn A Small fibers C Peripheral sensory Nerve fibers
Physiological Pain NOXIOUS STIMULUS INNOCUOUS STIMULUS A C fiber A DHN DHN PAIN INNOCUOUS SENSATION Touch Tactile Pressure First Pain Second Pain
Pain Afferent neurons A myelinated fiber C unmyelinated fiber Responds to noxious stimuli Both have free nerve endings Naciceptors (receptor Nyeri)
Nociceptors Mechanothermalnociceptors Respond to mechanical and thermal stimuli. display rapid conduction. Produced first pain and well localized. Ad fibers respond to this naciceptors. Polimodalnociceptors Respond to mechanical, thermal and chemical. Slow conduction. Produced second pain and diffuse. C fibers respond to this receptor. Exist in many tissues, skin, muscle, pariosteum, joints, and viscera, except brain.
Between noxious stimulus and perception of pain lies a complex series of electrophysioloc event, collectively termed NOCICEPTION4 physiologic processes are involved: 1. Transduction 2. Transmission 3. Modulation 4. Perception NOCICEPTION
Process whereby noxious stimuli are translated into electrical activity at the sensory endings of nerve TRANSDUCTION TRANSDUCTION Pressure Heat Chemical
Transduction Process Ca2+ K+ K+ Na+ 1. Transduction 3. Propagation 2. Spike Initiation 4. Transmitter Release Modified Meliala, 2006
NOCICEPTIVE PAIN Noxious Peripheral Stimuli Pain Autonomic Response Withdrawal Reflex Heat Cold Brain Intense Mechanical Nociceptor sensory neuron Force Heat Spinal cord Cold Modification Meliala, 2005
TRANSMISSION • Propagation of impulses throughout the sensory nervous system. Or • Passage of signal from periphery to the central NS.
Afferent Synaptic in DHN Substantia gelatinosa Marginal layer A Medial A C Lateral Nucleus proprius
MedulaSpinalis • Serabut-serabut Eksitatori • Serabut-serabut inhibitori MODULASI NYERI Dahulu: dikenalsebagai “SIMPLE RELAY STATION” UntuktransmisiNyeri Sekarang : Sebagaitempatinteraksi yang kompleksantara
SerabutEksitatori & Inhibitori Serabut Eksitatori Glutamate (Subs P) C Ad Glutamate + Ab OTAK Glutamate WDR & NS - Serabut Inhibitori GABA Glycine Opioids NA, 5HT
MODULATION • The process whereby endogenous analgesic system (opioid, serotonergic, and noradrenergic) can modify nociceptive transmission
Spinal Cord SPINAL CORD (DHN)is the key point of modulation • The place where afferent input is processed. • Where interaction between excitatory and inhibitory system. • NOCICEPTION IS BORN IN DORSAL HORN, BUT WE DON’T CALL IT PAIN TILL IT REACHES THE BRAIN (Dr. Ken Casey)
Descending Modulating Pathways Ascending pathways is modulated by descending modulating pathways in several higher centers; • CEREBRAL CORTEX • THALAMUS • MIDBRAIN/ BRAINSTEM • Periaqueductal gray (PAG) • Nuclei raphemagnus (NRM) • Locus ceruleus (LC) • Sub ceruleus • SPINAL CORD
SEROTONIN NEOREPINEPHRINE
Two Kind of Stimuli Nociceptor Noxious/ Innocuous Modulation DHN Facilitatory/ excitatory Inhibitory Pain No Pain Pain stimulus is not perfect terminology
Pain CNS Inhibition Excitation Nociception
Nociception Without Pain Pain X Inhibition Excitation CNS Example: Stress Induced Analgesia Nociception
Pain Without Nociception Pain Inhibition Excitation CNS X Example: Phantom ,neurophatic pain Nociception
Pain Perception Depends on the balance between: • Excitatory system • Inhibitory system (Cognitive, emotional, behavior)
Beecher Pain perception depend on the meaning of injury
Pain Perception Transduction Perception Pain Medulation Descending modulation Dorsal Horn transmission Dorsal root ganglion Ascending input Spinothalamic tract Peripheral nerve Trauma Peripheral nociceptors Adapted from Gottschalk A et al. Am Fam Physician. 2001;63:1981, and Kehlet H et al. Anesth Analg. 1993;77:1049.
Perception Final process to create the final subjective and emotional experience that we call pain Perception Pain Perception Brain How pain perception is processed, no body knows and Where pain perceptions in the brain still unclear.
What is nociceptive pain? • A sensory experience that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli • Can also be chronic (e.g. osteoarthritis) • Painful region is typically localized at the site of injury – often described as throbbing, aching or stiffness • Usually time-limited and resolves when damaged tissue heals (e.g. bone fractures, burns and bruises) • Responds to conventional analgesics
NOCICEPTIVE PAIN Noxious Peripheral Stimuli Pain Autonomic Response Withdrawal Reflex Heat Cold Brain Intense Mechanical Nociceptor sensory neuron Force Heat Spinal cord Cold Modification Meliala, 2005
TISSUE INJURY Prostaglandins Bradykinin Leukotriens PAIN Histamine NSAID (Cox1 or Cox2)
Prostaglandins produced in response to tissue injury; increase sensitivity of nociceptor (pain) Inflammation Tissue Painful stimulus Pain-sensitive tissue Prostaglandin Bloodvessel 1 Substance P Mast cell Histamine Bradykinin Substance P 2 3 Nociceptor 1 2 Nociceptor then releases substance P, which dilates blood vessels and increases release of inflammatory mediators, such as Bradykinin(redness & heat) 3 Substance P also promotes degranulation of mast cells, which release histamine(swelling)
Hyperalgesia Allodynia Sensitization 10 8 6 4 2 0 Normal Pain Response Injury Pain Intensity Hyperalgesia—heightened sense of pain to noxious stimuli Allodynia—pain resulting from normally painless stimuli Stimulus Intensity Gottschalk A et al. Am Fam Physician. 2001;63:1979-84.
CLINICAL PAIN (INFLAMATION PAIN) Low Intensity Stimulus Ab Fiber Ad Fiber PNS CNS Hyperexitable DHN DHN PAIN
What is neuropathic pain? • Pain caused by a primary lesion or dysfunction in the peripheral or central nervous system • Pain often described as shooting, electric shock-like or burning. • The painful region may not necessarily be the same as the site of injury. • Almost always a chronic condition (e.g. postherpetic neuralgia, poststroke pain) • Responds poorly to conventional analgesics