PERSISTANT DUCTUS ARTERIOSUS
PERSISTANT DUCTUS ARTERIOSUS. Lourdes Asiain M.D. October 2004. PERSISTENT DUCTUS ARTERIOSUS. Definition: Ductus arteriosus is a vessel that connects the pulmonary artery and aorta. Failure of closure and continued patency of fetal channel

PERSISTANT DUCTUS ARTERIOSUS
E N D
Presentation Transcript
PERSISTANT DUCTUS ARTERIOSUS • Lourdes Asiain M.D. October 2004
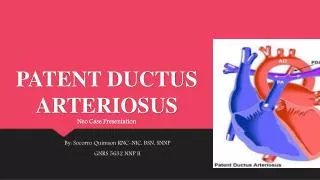
PERSISTENT DUCTUS ARTERIOSUS Definition: Ductus arteriosus is a vessel that connects the pulmonary artery and aorta. Failure of closure and continued patency of fetal channel is termed PERSISENT DUCTUS ARTERIOSUS (PDA)
HISTOLOGY PA/Aorta Ductus Cylindrical layers Spiral in opposing Directons Smooth Muscle Extracel matrix
PDA • In the fetus, the ductus diverts blood flow from the pulmonary circulation (high resistance) to the descending aorta. • An Increase in PaO2 constricts the ductus. Other factors, such as the release of vasoactive substances, contribute to the closure • Balance between constricting/relaxing substances
Absent Or reduced Increased Pa Oxygen (asphyxia, high Altitude) Factors Influencing closure of duct Contractile Apparatus Unresponsive Or deficient (prematurity, Genetic) Relaxant influences Prostaglandins
PDA • In full term healthy newborns, functional closure occurs in 50% by 24 hrs of age, in 90% by 48 hrs. • The effects of oxygen and prostaglandins vary at different gestational ages. • Oxygen has less of a constricting effect with decreasing gestational age • Indomethacin constricts the immature ductus more than the term ductus
PDA Factors assoc with increased incidence • Prematurity • RDS • Fluid overload • Asphyxia
PDA: Factors that increaseincidence Prematurity: Inversely related to gestational age Found in approx. 45% of infants <1750gm 80% of infants <1000gm
PDA: Factors that increaseincidence • RDS • Correlated with severity of RDS. • After surfactant treatment increased risk of clinically symptomatic PDA
PDA Factors associated with decreased incidence • Antenatal steroid administration • IUGR • Prolonged rupture of membranes
Clinical Signs • The clinical features assoc with L to R shunt depend on the magnitude of shunt and the ability to handle extra volume. • Shunt: magnitude and direction related to vessel diameter and pressure gradient between A and PA.
PDA: Clinical Signs • Murmur • Hyperactive precordium • Bounding peripheral pulses • Increase in pulse pressure • Hypotension • Respiratory deterioration
PDA: Management • Ventilatory support • Fluid restriction • Maintain hematocrit • Non surgical: Indomethacin (PGE1 inhib) Ibuprofen Transcatheter • Surgical: Ligation
PDA: Indomethacin • Prophylactic: 0.1mg/kg/dose q 24 hrs for 6 days • Symptomatic: <1250gm < 7 days >1250gm > 7 days Dose Prolonged: 4th,5th and 6th dose at 24 hr intervals
PDA: Indomethacin • Complications: Renal: decreased GFR GI Bleeding Platelet dysfunction Contraindicated if Creatinine >1.7mg, if patient is septic or if NEC present
Complications of PDA • CHF • Pulmonary hypertension • Aneurysm of duct (rare) • Thromboembolism (rare)
Conclusions • Common in preterm infants • Initial presentation usually DOL 1-4, Cardiopulmonary signs: murmur, bounding pulses, hyperactive precordium, resp deterioration. • Management: surgical non surgical
References • NeoFax 2004.17th edition.Thomas E. Young, MD and Barry Mangum . • Neonatology 5th edition.2004. Tricia Lacy Gomella. • Avery’s diseases of the Newborn. Taeusch et Ballard.