Download
1 / 35
360 likes | 714 Views
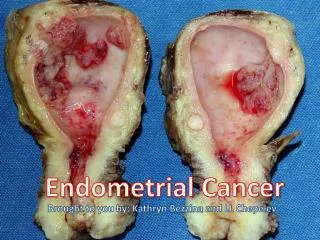
Endometrial Cancer: More Surgery, Less Radiation. Korean Society of Gynecologic Oncology and Colposcopy May 3, 2002 Larry J. Copeland, M.D. James Cancer Hospital Ohio State University. Endometrial Cancer. An Overview. 39,300 new diagnosis annually (US) 6,600 deaths annually

E N D
Endometrial Cancer:More Surgery, Less Radiation Korean Society of Gynecologic Oncology and Colposcopy May 3, 2002 Larry J. Copeland, M.D. James Cancer Hospital Ohio State University
Endometrial Cancer An Overview • 39,300 new diagnosis annually (US) • 6,600 deaths annually • most common female genital tract • malignancy • (Jemal et al CA Cancer J Clin, 52:23-47, 2002)
Endometrial Cancer • Pelvic and Aortic Nodes are at risk • for metastatic disease • Adjuvant treatment planninghas • relied heavily on prognostic profiling • of the uterus in an attempt to risk for • the presence of regional disease. • Why risk profiling when more • accurate information is available?
Endometrial Cancer: Risk ProfilingCervical Cancer Corollary The Cervical Cancer corollary would be to omit therapeutic lymphadenectomy, evaluate the surgical specimen (uterus/cervix) for prognostic factors (depth of invasion, size and LVS involvement, etc.) and decide on adjuvant radiation. We do not consider that to be acceptable therapy for cervical cancer - nor should we accept a similar treatment plan for endometrial cancer.
Endometrial Cancer: Risk Profiling Correlation of Grade and MI with Nodal Involvement
Endometrial Cancer Correlation of Grade and MI with Nodal Involvement
“Node Sampling” Unreliable for Diagnosis • Less than 30% of + nodes are palpable • (Creasman et al, Cancer 60:2035, 1987) • 37% of nodal metastasis are < 2 mm • (Girardi et al, Gynecol Oncol 49:177, 1993) • Intraoperative prediction by Gyn Onc • 36% false negative rate, sensitivity of 72% • (Arango et al, Obstet Gynecol 95:29, 2000)
Lymph Node Dissection versus Lymph Node Sampling Extent of lymphadenectomy correlates with survival (Kilgore et al, Gynecol Oncol 56:29, 1995) (COSA-NZ-UK, Int J Gynecol Cancer 6:102, 1996) Lymphadenectomy is the standard of care and decreases the need for external radiation therapy (Orr et al, Am J Obstet Gynecol 176:777, 1997) (Podratz et al, Gynecol Oncol 70:163, 1998)
Lymph Node Dissection versus Lymph Node Sampling Pelvic and Aortic node dissections improved survival and fewer retroperitoneal recurrences (Chuang et al, Gynecol Oncol 58:189, 1995) (Mohan et al, Gynecol Oncol 70:165, 1998) (Mariani et al, Gynecol Oncol 76:348, 2000) If Pelvic and Aortic nodes negative - no XRT (Gretz et al, Gynecol Oncol 61:409, 1996) (Orr et al, Am J Obstet Gynecol 176:777, 1997) (Berclaz et al, Int J Gynecol Cancer 9:322, 1999)
Adjuvant Radiation Therapy:External Pelvic Radiation • “Postoperative radiotherapy in stage I • endometrial carcinoma reduces local • recurrences but has no impact on overall • survival” • 3 Prospective randomized trials: • Aalders et al Obstet Gynecol 56:419, 1980 • Roberts et al (GOG) Abstr. Gynecol Oncol 68:135, 1998 • Creutzberg et al (PORTEC) Lancet 355:1404, 2000
Adjuvant Radiation Therapy: No Evidence of Survival Benefit • Aalders et al Obstet Gynecol 56:419, 1980 • Pelvic XRT5-Yr Surv.Death & Rec.Vag/PV Rec • Yes 89% 12.5% 2% • No 91% 12.3% 7% • _________________________________ • Issues: • No lymph node surgery, also vaginal cuff XRT given • 91% survival suggests selection of low risk population • High % of vaginal recurrences treated for cure
Adjuvant Radiation Therapy: No Evidence of Survival Benefit Roberts et al (GOG #99) Gynecol Oncol 68:135, 1998 Pelvic XRT5-Yr Surv.Vag/PV Rec Comp. Rate Yes 94% 2% 15% No 89% (NS) 12% 6% ____________________________________________________________________________________________________ Issues: Lymph node sampling, not lymphadenectomy (PLND) Intended to be intermediate risk - actually “low” risk population (18% grade 3) Prognostic subset analysis: XRT 87% vs 73% (P<0.01) (No surprise - High risk patients without PLND)
Adjuvant Radiation Therapy: No Evidence of Survival Benefit Creutzberg et al (PORTEC) Lancet 355:1404, 2000 Pelvic XRT5-Yr Surv.Vag/PV RecComp. Rate(G3/4) Yes 81% 4% 25% No 85% (NS)14% 6% ____________________________________________________________________________________________________ Issues: “Without routine LND”, Bx suspicious nodes Vag recurrence: 21% of XRT patients = NED @ 2yrs 79% of no XRT patients = NED @ 2yrs
Stage I with PLND and no EBRT: Evidence of Excellent Outcome • Orr et al, Am J Obstet Gynecol 176:777, 1997 • 444 patients: TAH/BSO/PV&PA LND • No teletherapy (EBRT) • Complications: Blood loss, infection, DVT • and surgical mortality similar to lesser Sx • Late complications: Lymphocele (1.2%), • leg edema (1.8%), hernia (2.9%) • Survivals: Stage IA 100%, IB 97%, IC 93% • Omission of XRT in SX Staged: Good Results
Pelvic Recurrences Vaginal recurrence: Prevented by brachytherapy, but 75% cured (Akerman et al Gynecol Oncol 60:177, 1999) (Nag et al, 2002 - peer review) Pelvic sidewall recurrences: Prevented with lymphadenectomy; possibly decreased by external beam radiation in unstaged patients but costly and complications high
Extrauterine Disease: Important to Identify Disease Significant percentage benefit from disease-directed local, systemic or combined therapy (15 - 50% extended survival) (Corn et al, Gynecol Oncol 56:29, 1995) (Gabriel et al, Int J Gynecol Cancer 8:397, 1998) (Selman et al, Int J Gynecol Cancer 8:423, 1998) (49% 5 yr survival stage IIIC with Chemo) (Katz et al, Am J Obstet Gynecol 184:1071, 2001) (McMeekin et al, Gynecol Oncol 81:273, 2001) (77% 3 yr survival stage IIIC with XRT, Chemo)
GOG122: Endometrial (Stage III/IV) Whole Abdomen Radiation Therapy I • Endometrial Cancer • Stage III/IV • No distant mets: • Aortic nodes negative • Aortic nodes unknown • Aortic nodes positive • with neg. scalene & • neg. CXR Cisplatin 50 mg/m2 Doxorubicin 60 mg/m2 II x 8 Open: 04-May-92 Closed: 25-Feb-98 Accrual: 389 pts Conclusions: Too early
Grade 1 Disease: Potential Trapfor Under Staging and Under Treatment • Thought to be a disease likely to be • treated satisfactorily with only • TAH/BSO • Reliability of assessment of grade and • myometrial invasion based on • preoperative and intraoperative • information is poor
Grade 1 Disease: Under Staging and Under Treating • Numerous studies support that at least • 20% of these patients are under staged • and under treated by surgery alone: • Malviya et al, Gynecol Oncol 34:299, 1989 • Goff et al, Gynecol Oncol 38:46, 1990 • Kucera et al, Gynecol Obstet Invest 49:62, 2000 • Petersen et al, Aust NZ J Obstet Gynecol 40:191,2000 • Mariana et al, Am J Obstet Gynecol 182:1506, 2000 • Orr et al, Current Opinion Oncology, 2001
Grade 1 Disease: Under Staging and Under Treating • Clear cell and serous variants may be at • increased risk for nodal disease in the • absence of myometrial invasion: • Takeshima et al J Obstet Gynecol 88:280, 1996 • Cirisano et al, Gynecol Oncol 77:55, 2000 • Gehrig et al, Obstet Gynecol 97:153, 2001 • Clear cell and serous component often • not diagnosed until postop path review
Correlation of Grade: D&C versus HysterectomySant Cassia et al, Gynecol Oncol 35,362, 1989 Hysterectomy GradeD&C Grade1 2 3 175% 20% 5% 2 23% 65% 11% 3 20% 35% 50%
Cost Considerations • Lymphadenectomy adds little to cost • (neither hospital stay nor morbidity) • Radiation therapy: External beam therapy • with or without brachytherapy = expensive • (Konski et al, Int. J Radiat Oncol Biol Phys 37:367, 1997)
Cost Considerations:Radiation Therapy (Konski et al, Int. J Radiat Oncol Biol Phys 37:367, 1997) Radiation RxApprox. Payor Cost LD Brachy (Cuff) $3500 Ext Beam (Whole pelvis) $4100 EBRT + Cuff $7200 High Dose Rate (Cuff) $5400 EBRT + HDR Cuff $9200
How Did We Get to This State of Affairs? (Compromised Treatment Plan) • Compare to Cervical Cancer - we do not accept avoidance of LND or sampling • Yet the risk and pathophysiology is similar to endometrial cancer • History: Evolution of Gyn Oncologist based on the “radical” procedures - radical hysterectomy and radical vulvectomy • Therapeutic management of regional nodes were a component of standard therapy for Cx & Vulva
How Did We Get to This State of Affairs? (Compromised Treatment Plan) • There is no controversy about the regional disease management for Cervix & Vulva - Radiation is reserved for clearly defined high risk metastatic disease or recurrence • How did we succumb to a distorted approach Endometrial Cancer?
How Did We Get to This State of Affairs? (Compromised Treatment Plan) • During the evolution of the discipline of Gynecologic Oncology, endometrial cancer required a primary surgical procedure (simple TAH/BSO), and radiation was an ingrained and accepted component of primary therapy. • Actually for years the primary therapy was preoperative radiation with surgery as the adjuvant therapy!
How Did We Get to This State of Affairs? (Compromised Treatment Plan) • It took decades to get over the problem of preoperative radiation - it was not until 1988 that the surgical staging of endometrial cancer was adopted. • Why did we change to surgical staging? • We had no idea as to the disease extent we were treating. Preoperative radiation was distorting - down staging - the disease features
How Did We Get to This State of Affairs? (Compromised Treatment Plan) • So how did we enter the process of lymph node sampling? This was evolving in the late 70’s early 80’s and it was the gynecologic oncologist’s idea! • What was the motivation - possibly debulking clinically suspect nodes • Why was lymph node dissection avoided - possibly to avoid the recognized complications of combining radiation with extensive surgery
Why Not Move On and Do It Correctly? • The data has evolved to support that every patient with endometrial cancer should undergo a pelvic and aortic lymphadenectomy and radiation should not be used in any surgically staged patient with disease limited to the uterus, regardless of prognostic profile of grade, MI, age, etc.
Why Did it Take So Long toFigure This Out? • The understanding of this disease, both the biology (risk of metastatic disease) and the role of adjuvant therapy has been compromised by incomplete data based upon incomplete surgical staging
We Need to Move Along! • But the data are now there and the modality of optimal treatment is not the issue now • The challenge now is the institution of the correct treatment • Turf is an inhibitor. Who does the surgery is not as important as to how well it is done!
We Need to Move Along! • Quality of lymphadenectomy: Honesty is needed. Pathology reports reflecting 1 or 2 nodes per pelvic or aortic node dissection is not a satisfactory surgical intervention. • Worse yet, nodules of fat do not constitute a lymphadenectomy
A Rad Onc Speaks! • Adjuvant XRT in EC … least satisfying… most patients do not benefit from XRT • Historic selection inadequate - unnecessary XRT treatment for many • “Women in my family … treated with comprehensive surgical staging … unless disease beyond uterus … adjuvant teletherapy would not be administered” Russell - Editorial, Gyn Oncol 84,191, 2002
Conclusions 1) All EC patients are at risk for nodal dz 2) Preop and intraoperative assessment of prognostic features are unreliable 3) All patients should have therapeutic pelvic and aortic lymphadenectomy 4) LND reduces need for adjuvant radiation 5) It is a serious challenge to our discipline to correct the current practice patterns