Download

1 / 47
470 likes | 847 Views
Why we need Root Canal Treatment ?. Aetiology of the pulp and periapical pathosis. Microbial : dental caries Mechanical : operative procedure (iatrogenic), trauma

E N D
Aetiology of the pulp and periapicalpathosis • Microbial: dental caries • Mechanical: operative procedure (iatrogenic), trauma • Chemical: pulpal (acid etching, bond), periapical (irrigation)
EFFECT OF DENTAL MATERIALS ON PULP • GIC – Well tolerated by pulp • Calcium hydroxide – includes dentin bridge formation. • Zine oxide – eugenol- has an anti-bacterial effect. • Formocresol – Cause chronic inflammation of the pulp. • Dentin bonding agent – can irritate the pulp causing inflammation www.rxdentistry.blogspot.com
myelinated A fibres (A-delta and A-beta fibres) Physiology of Pulpal PainOdontogenic pain coronal portion of the pulp and concentratedin the pulp horns sensibility of the dental pulp 2.Unmyelinated C fibres 2 types of sensory nerve fibres in the core of the pulpextend into the cell-free zone underneath the odontoblastic layer
Dentin tubule fluid movement Dehydration Heat Cold Hyper- osmoticsolutions Dentinal tubule and fluid Dentin A-delta fibers Odontoblast movement Sensory nerves
Location • Onset • Timing (frequency, duration) • Quality (sharp, dull, throbbing • Intensity (0-10) • Relieves/Aggravates • Associated symptoms Pain
The perception of pain in one part of the body that is distant from the actual source of the pain is known as referred pain. Referred Pain
Pulpal Status Vital Nonvital Normal Inflamed Necrotic Reversibly Inflamed Irreversibly Inflamed
Pulpal Pain • Deep, dull, aching pain of a threshold nature • Often difficult to localize • Occurs irrelevant to biomechanical(masticatory) functions
Common Characteristics of Pulpal Pain 1. Quality of pain is dull, aching, throbbing and occasionally sharp 2. An identifiable condition that reasonably explains the symptoms 3. Response to local noxious stimulation is proportionate and predictable 4. Pulpal pain tends to get better or worse, but rarely stays the same over time 5. Local anesthesia of the suspected tooth eliminates the pain
Site of Pain vs. Source of Pain • Site of Pain • The location where the patient feels the pain • Easily located by asking the patient to point out the region of the body that is painful • Source of Pain • That area of the body from which the pain actually originates
Primary Pain • Site (where it hurts) = Source (where it originates) • Eg./ cut finger • Heterotopic Pain • Site ≠ Source • Eg./ cardiac pain
Heterotopic Pain • Pain felt in an area other than its true site of origin (associated with deep, somatic pain). • Projected pain: perceived in the anatomic distribution of the same nerve that mediates the primary pain (painful adjacent teeth). • Referred pain: felt in an area innervated by a different nerve from the one that mediates the primary pain (teeth in opposing arch, face, head, neck). • Does not cross the midline. • Convergence of afferent neurons.
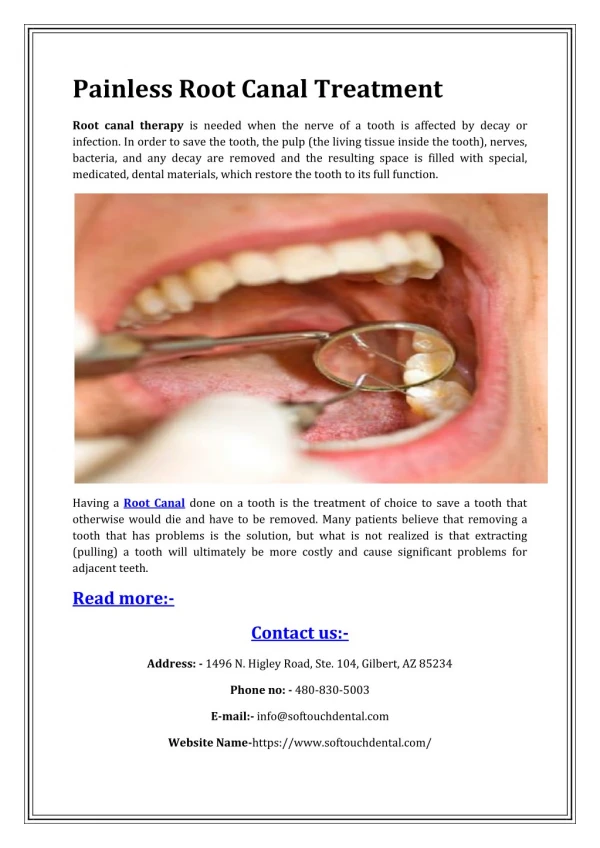
TERMINOLOGY • Dental pulp – Tissue within each tooth that contains the nerves, blood vessels, and cells that make the tooth a living organ • Pulpitis – A range of conditions from inflammation all the way to pulpal necrosis
TERMINOLOGY CON’T • Vitality– response of the pulpal tissue to a stimulus(healthy to nonresponsive) • Reversible/irreversible pulpitis– Reactions of a vital pulp to stimuli • Necrotic – death of the pulp • Periapical Tissue • chronic periodontitis • acute periodontitis
WHY PULPAL TESTING? Pulp testing is done to determine the treatment need of the tooth
PAIN • An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.
Acute Pain • Associated with tissue damage or injury. • Recent onset. • Limited duration. • Stimulation of peripheral and central nociceptors by algogenic substances (bradykinin, prostoglandin, leukotrienes, histamines, substance P, excitatory AAs).
Chronic Pain • Prolonged persistence of pain beyond the healing of tissue. • Frequently experienced in the absence of peripheral stimulation or lesions. • Result from changes in the dorsal horn and brain.
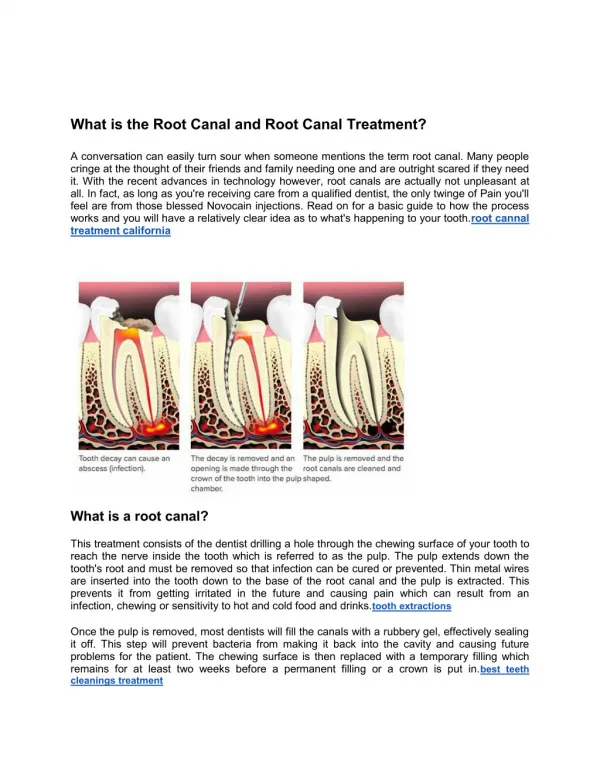
TOOTHACHE PAIN Toothache of odontogentic origin can be visceral (pupal) or musculoskeletal (periapical or periodontal). • When the pulp is exposed to a noxious stimulus, there is a reactive inflammatory response. • The resulting edema is unable to expand because of the surrounding inflexible cementum→ ↑ tissue pressure and ↓ blood flow that causes damaging effects to the pulp.
Considerations: • Healthy pulp (cellular) v Aged pulp (fibrous) • As an increasing amount of pulp tissue is involved, the inflammatory process progresses apically, until it extends out into the periapical tissue → apex becomes sensitive to palpation and percussion. • Periapical inflammation from non-pulpal causes can exhibit similar symptoms: • Hyperocclusion • Bruxism
Pulpal Status Vital Nonvital Normal Inflamed Necrotic Reversibly Inflamed Irreversibly Inflamed
CLINICAL CLASSIFICATION OF PULPALAND PERIAPICAL DISEASES • Normal Pulp • Reversible Pulpitis • Irreversible Pulpitis • Necrosis Pulpal Disease
PAIN • Location • Onset • Timing (frequency, duration) • Quality (sharp, dull, throbbing, aching,burning, etc.) • Intensity (0-10) • Relieves / Aggravates • Associated symptoms
Reversible Pulpitis Common causes: • Caries, recent restorative procedures, faulty restorations, trauma, exposed dentinal tubules, periodontal scaling.
Condition should return to normal with removal of the cause. • Pulpal recovery will occur if reparative cells in the pulp are adequate.
Remove irritant if present (caries; fracture; exposed dentinal tubules). • If no pulp exposure: CaOH, restore, monitor • If pulp exposure: • Carious: initiate RCT • Mechanical: >1 mm: initiate RCT <1 mm crown planned: initiate RCT <1 mm: direct cap or RCT • If recent operative or trauma – postpone additional treatment and monitor.
Pulpalinflamation and degeneration not expected to improve. • A physiologically older pulp has less ability to recover due to decrease in vascularity and reparative cells. • As inflammation spreads apically, cellular organization begins to break down. • Localized pressure slows venous return, resulting in buildup of toxins and lower pH that causes widespread cellular destruction.
Treatment of Irreversible Pulpitis Ideal immediate treatment • (complete removal of pulpal tissue)completely relieve occlusion if have acute periapicalperidontitis.
Pulpal Disease Necrotic Pulp
Necrotic Pulp • Results from continued degeneration of an acutely inflamed pulp. • Involves a progressed breakdown of cellular organization and no reparative potential. • Commonly have apical radiolucent lesion. (always conduct proper pulp testing to rule out a non-pulpal origin). • With multi-rooted teeth, one root may contain partially vital pulp, whereas other roots may be nonvital (necrotic).
Treatment of Necrotic Pulp Minimum immediate treatment (if not extraction) • Partial instrumentation of canals: • Place Ca(OH)² into all canals • completely relieve occlusion if have acute apical periodontitis. Ideal immediate treatment • Complete instrumentation of canals: • completely relieve occlusion if have acute apical periodontitis.