Download
1 / 25
280 likes | 667 Views
B alloon-pump assisted C oronary I ntervention S tudy BCIS-1. Simon Redwood St Thomas’ Hospital / King’s College London On behalf of the BCIS-1 Investigators. Steering Committee: Divaka Perera , Rod Stables, Jean Booth, Martyn Thomas. Potential conflicts of interest.

E N D
Balloon-pumpassisted Coronary InterventionStudyBCIS-1 Simon Redwood St Thomas’ Hospital / King’s College London On behalf of the BCIS-1 Investigators Steering Committee: DivakaPerera, Rod Stables, Jean Booth, Martyn Thomas
Potential conflicts of interest Speaker’s name: Simon Redwood √I do not have any potential conflict of interest This trial was supported by unrestricted grants from: Datascope/ Maquet Eli Lilly Cordis 1
Trial Organization • Steering Committee • Divaka Perera, Rod Stables, Martyn Thomas, Jean Booth, Simon Redwood • Clinical Events Committee • James Cotton, Nick Curzen, Adam de Belder, David Roberts • Data Monitoring and Safety Committee • Peter Ludman (Chair) , Gerald Stansby, Chris Palmer • Clinical Trials and Evaluation Unit • Jean Booth, Fiona Nugara, Marcus Flather, Charlotte Gillam, Michael Roughton, Winston Banya
Elective vs provisional IABP in high-risk PCI P = 0.01 • 133 pts EF <30, elective PCI • Elective IABP, 61 pts. Jeopardy Score 8.0 + 2.8 • Provisional IABP, 72 pts. Jeopardy Score 6.7 + 2.4 (p=0.008) Correlates of MACE Odds Ratio Elective IABP 0.11 Jeopardy Score 5.37 % P = 0.29 Briguori et al, AHJ 2003;145:700-7
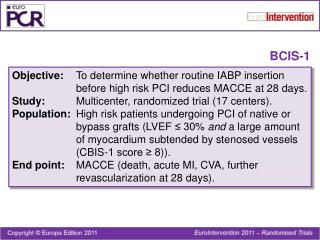
Balloon-pump assisted Coronary Intervention Study • Objectives: • To compare the efficacy and safety of elective Intra-Aortic Balloon Pump (IABP) insertion prior to high-risk PCI vs. conventional treatment (with no planned IABP use) • Structure: • Prospective, open, randomized trial • 17 UK centres • n=300 (150 in each arm) • Sample Size = 274 pts (predicted MACCE 5% vs. 15%, β=80%, α= 5%)
LVEF < 30% Jeopardy Score ≥ 8 Randomize Elective IABP Insertion No Planned IABP PCI Remove IABP 4-24 hrs after PCI Hospital Follow-up To discharge or 28 days 6 month follow-up
BCIS-1 • Primary Outcome Measure • Major Adverse Cardiovascular or Cerebral Events (MACCE) at hospital discharge or 28 days (whichever is sooner), including • All-Cause Death • Acute MI • Further revascularization by PCI or CABG • CVA Perera et al AHJ 2009; in press
Secondary Outcome Measures • Six month mortality • Procedural complications • Prolonged hypotension OR • VT/VF requiring cardioversion OR • Cardiac arrest requiring CPR/ventilation • Bleeding complications • Vascular complications • Procedural success • Duration of hospital stay
Study DefinitionsMyocardial Infarction • < 72 hrs post PCI, baseline CKMB normal • CKMB > 3x ULN • < 72 hrs post PCI, baseline CKMB high • CKMB > 1.5 x baseline • > 72 hrs post PCI • Elevated Tn with symptoms or ECG changes • < 72 hrs post CABG • CKMB > 5 x ULN and new Q waves or LBBB • Sudden Death • Cardiac Arrest with ST elevation/LBBB and/or evidence of thrombus at autopsy/angiography
Study Definitions • Prolonged Hypotension • 1. Elective IABP • MAP <75 mmHg for >10 mins despite fluids OR new inotropes to maintain MAP >75mmHg • 2. No Planned IABP • As above OR insertion of IABP to maintain MAP >75mmHg • Major bleed • >4g/dl drop in Hb • Minor bleed • 2-4g/dl drop in Hb
Inclusion Criteria • Impaired LV function (EF < 30%) and • Extensive Myocardium at Risk • BCIS-1 Jeopardy Score > 8 • or...Target vessel supplying occluded vessel which supplies >40% of myocardium
Jeopardy Score 6 Major Coronary Segments 2 points for each lesion + 2 for each territory distal to lesion 2 2 2 2 2 2 Califf et al JACC 1985;5:1055-63
Jeopardy Score BCIS-1 Allows LM and Graft Classification 6 Major Coronary Segments 2 points for each lesion + 2 for each territory distal to lesion Negative points for functioning grafts 2 2 2 2 2 2 Perera et al AHJ 2009; in press
Exclusion Criteria • Cardiogenic Shock • Systolic BP <85 mmHg despite correction of hypovolemia • Acute MI < 48 hours before randomization • Planned staged PCI within 28 days • Complications of acute MI • VSD, severe MR or intractable VT/VF • Contraindication to IABP
BCIS-1 Recruitment Completed 21st Jan 09 Total 301 patients
Components of the Primary Outcome: MACCEto Hospital Discharge/ 28 days * Cox regression † Hierarchical 1 patient had MI and died; 2 patients had MI and PCI
Major Secondary Outcomes †2 test * Fisher’s exact test
Kaplan Meier 6 month mortality 7.3% vs 4.6%, p = 0.32 Elective IABP No Planned
IABP Use in No Planned Group • IABP inserted as ‘bailout’ in 18 patients (12%) • hypotension in 13 (72%) • Pulmonary oedema in 1, vessel closure in 1 • In these patients: • EF 24.4 + 5.5 % • Jeopardy Score 11.2 + 1.4 ; JS 12 in 13 pts (72%) • Duration of IABP: median of 22.9 hrs (vs 8.6 hrs in elective group) • MACCE occurred in 4 patients (22%)
Conclusions BCIS have performed the first randomized trial of elective vs. ‘bailout’ IABP in patients with poor LV function and severe coronary disease We did not find evidence that Elective IABP to support high risk PCI is associated with a reduction in MACCE at hospital discharge 12% in the no-planned group required emergency IABP, supporting the important role of provisional IABP use Patients with poor LV function and severe coronary disease treated by PCI appear to have acceptable in-hospital and 6 month mortality (1.3% and 6%)