Download
1 / 30
330 likes | 1.06k Views
Carvedilol Prophylaxis in Anthracycline-Induced Cardiomyopathy . Yim de Guzman COH Medicine Rotation Western University of Health Sciences College of Pharmacy March 24, 2010. Objectives. Patient case discussion Pathophysiology of anthracycline-induced cardiomyopathy

E N D
Carvedilol Prophylaxis in Anthracycline-Induced Cardiomyopathy Yim de Guzman COH Medicine Rotation Western University of Health Sciences College of Pharmacy March 24, 2010
Objectives • Patient case discussion • Pathophysiology of anthracycline-induced cardiomyopathy • Potential prevention strategies • 2008 ASCO guideline • Carvedilol as potential prophylactic treatment • Conclusion
Patient Presentation • CR is a 31 yo Caucasian male with hx of neuroblastoma at age of 1½ yo, starting chemotherapy with cytarabine and idarubicin 7+3 for recently diagnosed acute myelogeous leukemia • HPI • C/O abdominal discomfort 10 days prior • Recent elbow, wrist, knuckle, shin and ankle pain • Episode of sweating on 3/2/2010 • More tired than usual, increased sleep and headaches • Pancytopenia: WBC 1.7, Hgb 9.7, platelet 34,000 • Bone marrow biopsy: + AML • Admitted to COH on 3/3/2010
Patient Presentation • PMH • Neuroblastoma: had surgery followed with 6 months of chemotherapy and radiation therapy to lower abdomen • Pyloric stenosis as an infant • SH • Quit smoking 2 years ago, prior had 10 years smoking history • Drinks alcohol occasionally • No history of IV drug use • Works full time for UPS as driver • FH • Maternal aunt dx with ovarian and uterus CA • Maternal grandfather dx with some types of CA • Has one half sister and one full sister (match donor)
Patient Presentation • Current meds • Cytarabine 100 mg/m2 daily on d1-7 • Idarubicin 12 mg/m2 daily on d1-3 • Acyclovir 400mg BID • Allopurinol 300mg daily • Protonix 40mg daily • Allergies • NKA
Laboratory Values • Labs • WBC 1.8, H/H: 9.5/26.8, platelet 35, peripheral blasts 12%, • Tests • Echocardiogram on 3/4/2010 • EF=64%
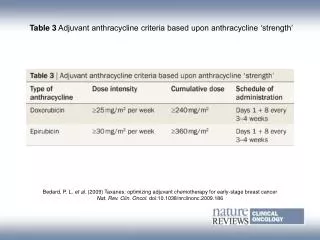
Clinical question • Cardiomyopathy risk in CR • Unknown chemotherapy received as child • Common chemo regimen for neuroblastoma: daunorubicin/doxorubicin, cyclophosphamide, carboplatin/cisplatin, and epotoside • Current idarubicin regimen • Cumulative dose=36mg/m2 • 5% risk of cardiomyopathy at cumulative dose of 150mg/m2 -290mg/m2(1) • Potential need for further AT therapy • Is carvedilol an effective prophylactic treatment for AML patient against anthracycline-induced cardiomyopathy?
Pathophysiology of Anthracycline-Induced Cardiomyopathy • Anthracyclines are potent antineoplastic agents • Associated with irreversible cardiomyopathy • Chronic Heart failure (5%)2 • Over 50% of pt treated with AT will have varying degree of cardiomyopathy over 10-20 years post therapy2 • Toxicity can occur at any stage of treatment • Acute • During administration of AT therapy • Early • Several days to months following AT therapy • Delayed • Years to decades following AT therapy Cardinal D. J Am Coll Cardiol. 2010 Jan 19;55(3):213-20.
Pathophysiology of Anthracycline-Induced Cardiomyopathy • Myocytes damage • Free oxygen radicals • Lipid peroxidation of membrane • Apoptosis • Redox activation to a semi-quinone intermediate • Generate superoxide and hydrogen peroxide • Mitochondrial dysfunction • Decrease mitochondrial Ca++ loading capacity http://www.heartandmetabolism.org/issues/HM35/HM35basicartic.asp
Risk Factors of AT-induced cardiomyopathy • Cumulative dose • Patient age • Older and younger pts have increased risk at lower AT doses • Preexisting cardiac dysfunction, hypertension • Radiation therapy • Prior mediastinal radiation • Endothelial cell damage • Compromise coronary artery blood flow • Concurrent chemotherapy • Taxanes • Trastuzumab • HSCT • Cyclophosphamide • TBI
Prognosis • Anthracycline-induced cardiomyopathy has poorer prognosis compared to other forms of cardiomyopathy • 2 year mortality rate of up to 60% (Cardinale)
Potential Strategies for AT-CMP Prevention • Administration modifications • Structural modifications • Coenzyme Q10 • Vit A, Vit C and Vit E • Dexrazoxane • Carvedilol
Potential Strategies for AT-CMP Prevention Wouters KA. Br J Haematol. 2005 Dec;131(5):561-78
Potential Strategies for AT-CMP Prevention Wouters KA. Br J Haematol. 2005 Dec;131(5):561-78
Dexrazoxane • EDTA-like chelator • Bind iron that is release from intracellular storage secondary to lipid peroxidation, acting as cofactor for free radicals • Data from meta-analysis: Cardioprotective interventions for cancer patients receiving anthracyclines • 9 RCTs • 692 adult patient received dexrazoxane • 711 adult patient in control group (either placebo or nothing) • 8 studies: solid tumors with majority being breast cancer • 1 study: leukemia • Occurrence of HF • (RR) = 0.28, 95% CI (0.18 to 0.42) P<0.00001 • Response rate • RR = 0.88, 95% CI (0.77 to 1.01) P = 0.06 • Patients treated with dexrazoxane might have a lower anti-tumor response rate • Meta-analysis of survival showed no significant difference between the dexrazoxane and control group • Conclude that if the risk of cardiac damage is expected to be high, it might be justified to use dexrazoxane in patients with cancer treated with anthracyclines. Dalen E. Cochrane Database Syst Rev 2005;(1): CD003917
ASCO Guideline 2008 • Use in adult patients with other malignancies: • Use of dexrazoxane can be considered in adult patients who have received more than 300mg/m2 of doxorubicin-based therapy • Caution should be exercised in the use of dexrazoxane in settings in which doxorubicin-based therapy has been shown to improve survival Hensley ML. J Clin Oncol. 2009 Jan 1;27(1):127-45.
Carvedilol • Adrenergic blockade • Non-selective Beta-blocker • FDA approved for • Heart failure • Hypertension • Impaired left ventricular function – Myocardial infarction • Non-FDA labeled indications • Chronic angina • Atrial arrhythmia • Cardiac dysrhythmia • Congestive cardiomyopathy • CHF, nitrate tolerance • Disease of liver • Prophylaxis for gastroesophagealvarices • Surgical procedure
Carvedilol • Proposed mechanism for prevention of AT-induced cardiomyopathy • Potent anti-oxidant • 10x more potent than alpha-tocopherol • Metabolites 1,000 more potent • Accumulates in myocardium plasma membrane • 10,000x more in cell membrane than in extracelluar medium • Inhibit formation of reactive oxygen radicals • Prevent lipid peroxidation • Prevent formation of vacuoles • Scavenger for oxygen free radicals • Prevent depletion of endogenous anti-oxidants • Vit E • Glutathione Matsui H. Life Sciences Life Sci. 1999;65(12):1265-74. Spallarossa P. Journal of Molecular and Cellular Cardiology 37 (2004) 837–846
AT-induced cardiac myocyte in rat model Fig B: Light micrograph of doxorubicin-treated rat cardiac myocytes Fig A: Light micrograph of normal cardiac myocyte Fig C: Light micrograph of doxorubicin and carvedilol treated rat cardiac myocytes Santos DL. Toxicology and Applied Pharmacology 185, 218-227
RCT: Protective effects of carvedilol against anthracycline-induced cardiomyopathy • Patient diagnosed with malignancy and planned AT therapy with doxorubicin or epirubicin • Exclusion criteria: • Previous chemotherapy or radiotherapy • Presence of CHF symptoms or established CMP • Hx of CAD • Presence of moderate to severe mitral or aortic valve disease • Any CI to carvedilol • Bundle branch block • Thyroid function disorder • Other comorbid disease • Taking other drugs that affect cardiac function
RCT: Protective effects of carvedilol against anthracycline-induced cardiomyopathy • Design of study • Randomized • Single-blinded • Placebo-controlled • Arms of study • 25 patients received 12.5mg once daily carvedilol before start of CT • 25 patients received placebo • Duration • 6 months during CT • Primary end point • Systolic function
RCT: Protective effects of carvedilol against anthracycline-induced cardiomyopathy Kalay N. J Am Coll Cardiol. 2006 Dec 5;48(11):2258-62.
RCT: Protective effects of carvedilol against anthracycline-induced cardiomyopathy • Carvedilol group mean EF: 70.5 vs. 69.7, respectively; p=0.3 • Control group mean EF: 68.9 vs. 52.3; p=0.001 Kalay N. J Am Coll Cardiol. 2006 Dec 5;48(11):2258-62.
RCT: Protective effects of carvedilol against anthracycline-induced cardiomyopathy Kalay N. J Am Coll Cardiol. 2006 Dec 5;48(11):2258-62.
RCT: Protective effects of carvedilol against anthracycline-induced cardiomyopathy • Results • Primary outcome: Heart failure (EF < 50%) • 1 (4%) pt from carvedilol group developed HF • 5 (20%) pt from control group developed HF • ARR=16%, RRR=80%, NNT=6 • Systolic diameters • Carvedilol group: 31.4 ± 5.4 mm vs. 32.2 ± 6.6 mm; p 0.7 • Control group: 30.3 ± 5.2 mm vs. 38.0 ± 5.3 mm; p 0.0001 • Diastolic diameters • Carvedilol group: 47.6 ± 5.6 mm vs. 47.4 ± 3.7mm; p 0.8 • Control group: 45.6 ± 5.0 mm vs. 50.9 ± 5.6 mm; p 0.008
Limitations • Limited number of enrolled patients-low power • Found less mortality in carvedilol group but was not significant • Only evaluated early cardiotoxic effect of AT • Early CMP depend on cumulative dose of AT • Late CMP can occur to patient with any dose • Most patient were solid tumor with other types not specified • Patient were blinded but clinicians were not blinded
Carvedilol ADR • Cardiovascular: bradyarrhythmia, hypotension peripheral edema, atrioventricular block • Endocrine metabolic: hyperglycemia, weight gain • Gastrointestinal: diarrhea • Neurologic: dizziness • Reproductive: erectile dysfunction • Other: fatigue
Conclusion • Carvedilol ppx in AT therapy show promising protective effect against cardiomyopathy • However, need larger randomized trial to further investigate the protective effect
Back to CR • May be an option for CR • Young without added risk factors • Unclear on cumulative dose of AT • Future need for further AT therapy • Confirmed persistent AML with >70% blast in marrow post induction regimen • Avoid possible malignant protective effect from Dexrazoxane
References • Anderlini P, Benjamin RS, Wong FC, et al. Idarubicin cardiotoxicity: a retrospective study in acute myeloid leukemia and myelodysplasia.J Clin Oncol. 1995 Nov;13(11):2827-34. • Cardinale D, Colombo A, Lamantia G, et al. Anthracycline-induced cardiomyopathy: clinical relevance and response to pharmacologic therapy. J Am Coll Cardiol. 2010 Jan 19;55(3):213-20. • Dalen E; Caron H; Dickinson H; Kremer L. Cardioprotective interventions for cancer patients receiving anthracyclines. Cochrane Database Syst Rev 2005;(1): CD003917 • Hensley ML; Hagerty KL; Kewalramani T; et al. American Society of Clinical Oncology 2008 clinical practice guideline update: use of chemotherapy and radiation therapy protectants. J Clin Oncol. 2009 Jan 1;27(1):127-45. • Kalay N; Basar E; Ozdogru I; et al. Protective effects of carvedilol against anthracycline-induced cardiomyopathy. J Am Coll Cardiol. 2006 Dec 5;48(11):2258-62. • Matsui H, Morishima I, Numaguchi Y, et al. Protective effects of carvedilol against doxorubicin-induced cardiomyopathy in rats. Life Sci. 1999;65(12):1265-74. • Santos DL, Moreno AJ, Leino RL, et al. Carvedilol protects against doxorubicin-induced mitochondrial cardiomyopathy. Toxicol Appl Pharmacol. 2002 Dec 15;185(3):218-27. • Wouters KA, Kremer LC, Miller TL, et al. Protecting against anthracycline-induced myocardial damage: a review of the most promising strategies. Br J Haematol. 2005 Dec;131(5):561-78. Review.