Download
1 / 16
160 likes | 184 Views
Study evaluates ACE-i and β-blocker effect on HER2+ breast cancer patients receiving trastuzumab, with lisinopril and carvedilol showing efficacy in preventing cardiotoxic events.

E N D
Lisinopril or Carvedilol for Prevention of Trastuzumab Induced Cardiotoxicity Maya Guglin, MD, PhDUniversity of Kentucky, Lexington, KY Jeffrey Krischer, PhDUniversity of South Florida, Tampa, FL Roy Tamura, PhDUniversity of South Florida, Tampa, FL Angelina Fink, MPHH. Lee Moffitt Cancer, Tampa, FL Lauren Bello-Matricaria University of South Florida, Tampa, FL Worta McCaskill-Stevens, MDNational Cancer Institute, Rockville, MD Pamela N. Munster, MD University of California San Francisco, San Francisco, CA • ClinicalTrials.gov Identifier:NCT01009918 • Sponsors and Collaborators: University of South Florida National Cancer Institute
Introduction:Incidence of Cardiotoxicity Seidman et al. J Clin Oncol 2002; 20:1215-1221:
Hypothesis HER2 positive breast cancer patients starting Trastuzumab ACE-I Placebo β-blocker EF ↓ EF EF
Methods • Proportion of cardiotoxicity events at the end of trastuzumab therapy or week 52 was analyzed both by a chi-square test and by logistic regression with anthracycline strata and baseline LVEF as independent factors. • The significance of the coefficients was determined by the Wald test. • Long term cardiotoxicity effects, a secondary outcome, were analyzed by proportional hazards analyses of the time to first cardiotoxicity event were conducted with treatment group, anthracycline strata and baseline LVEF as independent factors of the model.
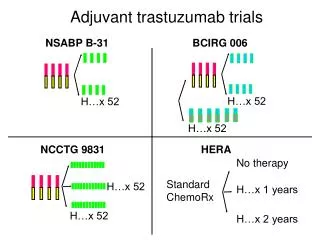
Design Trastuzumab Enrollment + anthracyclines - anthracyclines Randomization ACE-I β-blocker ACE-I β-blocker Placebo Placebo
Primary Objective to determine if administration of lisinopril or carvedilol results in decrease of the rate of cardiotoxicity in comparison with placebo
Secondary Objectives to determine whether participants receiving lisinopril or carvedilol experienced fewer interruptions in trastuzumab therapy to determine if treatment effects were consistent in anthracycline and non-anthracycline cohorts.
Inclusion Criteria Age ≥18 years old HER2 positive breast cancer Scheduled to receive adjuvant trastuzumab therapy LVEF ≥ 50% by MUGA scan or echocardiogram, based on institutional/clinician preference Normal renal and hepatic function Systolic blood pressure of > 90 mmHg Heart rate ≥ 60 beats/minutes
Exclusion Criteria Current treatment with ACE-inhibitors, ARBs, ß-blockers, digoxin Patients with metastatic disease Known cardiac history History of asthma or related bronchospastic conditions Hereditary or idiopathic angioedema Severe hypersensitivity reaction to drugs or other causes Pregnant or breastfeeding (must use effective birth control)
Definition of Cardiotoxicity Decrease from baseline of ≥10% (LVEF) at study follow-up or An absolute decrease ≥ 5% in LVEF if it is < 50% at study follow-up The determination of LVEF was made locally at each site. LVEF testing was conducted at baseline, 3, 6, 9, and 12 months.
Results • 468 patients • 127 participating sites • 86.3% Caucasian, 7.3% African American, • mean age 51±10.7 • Baseline LVEF 63±6.29% • No difference between arms
Cardiotoxicity-free survival for the cohort with Trastuzumab and anthracycline exposure
Cardiotoxicity-free survival for the cohort with Trastuzumab exposure without anthracyclines
Conclusions • In patients with HER2 positive breast cancer treated with trastuzumab, the cardiotoxic events were similar on placebo, lisinopril or carvedilol with comparable treatment interruptions. • Both lisinopril and carvedilol were effective in preventing cardiotoxicity in patients who were treated with both trastuzumab and anthracyclines. • Cardiotoxicity associated with Trastuzumab superimposed on prior or current exposure to anthracyclines can be prevented with lisinopril or carvedilol. • In high risk patients who may benefit from an anthracycline-containing regimen, the use of lisinopril or carvedilol is justified and should be considered to off-set cardiotoxic events by the use of anthracyclines in combination with trastuzumab.