Download
1 / 21
210 likes | 339 Views
The Hemostatic System as a Modulator of Atherosclerosis. Borissoff , Julian I., Henri M. Spronk , and Hugo Ten Cate . New England Journal of Medicine 2011; 364:1746-760. Ashley Harrison University of Georgia PharmD Candidate 2012 Discussion. Level of Evidence. Introduction.

E N D
The Hemostatic System as a Modulator of Atherosclerosis Borissoff, Julian I., Henri M. Spronk, and Hugo Ten Cate. New England Journal of Medicine 2011; 364:1746-760. Ashley Harrison University of Georgia PharmD Candidate 2012 Discussion
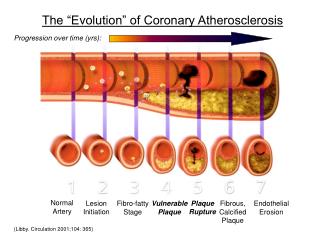
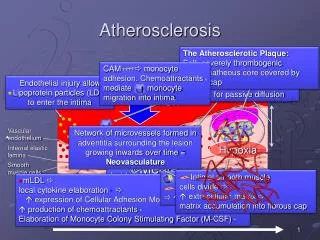
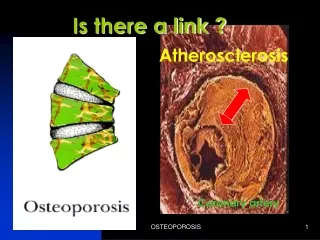
Introduction • Classically, the onset and progression of atherosclerosis is related to inflammation • Macrophages, neutrophils, and lymphocytes play a pivotal role in destabilizing and rupturing atherosclerotic plaques, resulting in atherothrombosis • However, there has been recent linkage of the inflammation and coagulation in atherosclerosis • While antiplatelet/anticoagulant therapy has not been shown to produce regression of plaques, the hemostatic modulators influence the composition of the arterial wall.
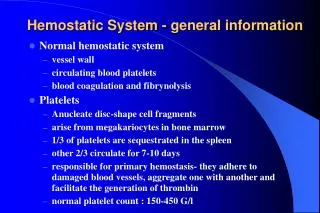
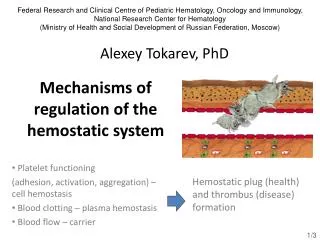
Linking the Hemostatic System with Atherosclerosis • Hemostasis: slowed blood flow • Due to… • Normal vasoconstriction • Abnormal obstruction (plaques) • Coagulation/surgical means (ligation) • The goal is to achieve an equilibrium that allows for proper blood flow and to stop bleeding after vascular injury. • When this balance is disrupted, it can lead to thrombus formation or bleeding
Linking the Hemostatic System with Atherosclerosis: Responses in the Vasculature • Aside from their traditional hemostatic role, platelets are also important in pro-inflammatory conditions such as atherosclerosis • Coagulation proteins are involved in disrupting the endothelial barrier, leukocyte recruitment, inflammation, migration and proliferation of VSMCs, and angiogenesis • Most of these actions are mediated by the TF-FVIIa complex, factor Xa, and thrombin and involve protease-activated receptors (PARs). • PARs are located on vascular cells normally. However, in atherogenesis these receptors are overexpressed
Linking the Hemostatic System with Atherosclerosis: Platelets • When inflammation is present, the vascular endothelium changes to a proatherogenic phenotype (regardless of vascular wall injury) • As a result, cell-adhesion molecules such as P-selectin are enhanced on the surface of both platelets and endothelial cells. The up-regulation of P-selectin causes platelets to interact with circulating leukocytes, which is critical in plaque formation and progression • At the same time, platelets adhere to the endothelium primarily via vWF, causing them to secrete atherogenic mediators: cytokines, chemokines, adhesion molecules, coagulation factors, etc.
Normal Vascular Endothelium • Intact endothelium has an anticoagulant phenotype • Circulating platelets and clotting factors do not significantly adhere
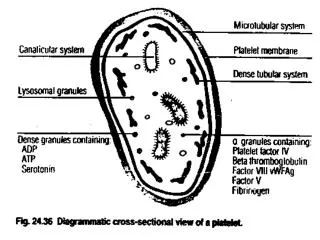
Damaged Vascular Endothelium • Vascular injury exposes subendothelial matrix proteins (collage, von Willebrand factor) and changes to a procoagulant phenotype • Matrix proteins cause platelet adherence and activation and subsequent secretion of… • ADP: induces platelet aggregation • TXA2: plt. activator and vasoconstrictor • 5-HT: vasoconstrictor and plt. aggregation • This results in platelets binding to fibrinogen and cross-linking to other platelets– “platelet plug”
Linking the Hemostatic System with Atherosclerosis:The Coagulation System During Plaque Progression • Coagulation proteins have been linked to atherogenesis by increased thrombin-generating activity in early atherosclerotic lesions • The increased presence of these coagulation factors in early atherosclerotic vessels will eventually contribute plaque instability • Also, clinical studies have shown that a more fibrous plaque structure (rather than a lipid-rich structure with inflammatory cells) is associated with thrombin generation in coronary artery stenosis patients
Extrinsic Pathway: Tissue Factor Pathway • Tissue factor is considered to be the primary starting point of the coagulation pathway • TF is found to be higher in atherosclerotic lesions from patients with unstable angina or MI vs. those with stable conditions • Factor VII forms a complex with TF, which takes part in: vascular remodeling, angiogenesis, chemotaxis, and inflammation. • Plasma levels of TF antigen are associated with markers of subclinical atherosclerosis (increased carotid intima-media thickness) and increased risk of CV-related death
Intrinsic Pathway: Contact Activation Pathway • While this pathway is not essential in hemostasis, it may be involved in arterial thrombosis • Negatively charged surfaces in blood trigger the cleavage of factor XII, which activates proinflammatory kallikrein-kinin and complement. • Factor XII-mediated formation of bradykinin regulates vasodilation and vascular permeabilities as well as induces complement activation. • Levels of kallikrein in tissue and prekallikrein in plasma have been associated with CVD severity • If factor XII and the kallikrein-kinin system are stimulated over a period of time, this may encourage a proatherogenic environment
The Common Pathway • The intrinsic and extrinsic pathways both activate factor X to Xa • Factor Xa signals various cell types of the CV system– this contributes to the production of proinflammatory cytokines, cell-adhesion molecule expression, and up-regulation of TF • These signals may contribute to the progression of atherosclerotic plaques by causing inflammation, migration of leukocytes, and angiogenesis • An important pharmacologic finding is that factor Xa inhibitors reduced vascular remodeling and neointimal formation
The Common Pathway:Thrombin • Under normal circumstances, thrombin binds to thrombomodulin to enhance the activation of protein C, an endogenous anticoagulant and antiinflammatory. • During atherogenesis, thrombomodulin decays allowing thrombin to potentiate endothelial dysfunction, oxidative stress, inflammation, and activation of platelets and leukocytes. • Thrombin (along with factors Xa, XIa, IXa, and plasmin) also cleaves complement proteins C3 and C5 which induce inflammation and chemotaxis of inflammatory cells. • Furthermore, Melagatran (a direct thrombin inhibitor) reduces progression of atherosclerosis and promotes plaque stability by inhibiting proinflammatory transcription factors • This effect shows a cross-linking between coagulation and inflammation in atherosclerosis
The Common Pathway:Fibrinogen and Fibrin • Plasma fibrinogen levels are a major indicator of the amount of formed thrombin. • In the presence of thrombin, fibrinogen is converted to fibrin, forming a fibrin clot • The effects of fibrinogen on the plaque phenotype… • Favors permeability of endothelial cells, accumulation of LDL, and formation of foam cells • Induces monocyte and VSMC migration • Increases platelet reactivity and aggregation • Enhances inflammation
The Common Pathway:Factor XIII • Factor XIII is also known as “fibrin stabilizing factor” because it cross-links fibrin to form fibrin chains, creating an insoluble clot • Factor XIII also enhances the formation of angiotensin II receptors, worsening atherosclerosis by continually sensitizing circulating monocytes and enhacing inflammation.
Anticoagulation Pathways in Vascular Inflammation:TFPI • Tissue Factor Pathway Inhibitor (TFPI) acts on factor VIIa and Xa to decrease thrombin formation, resulting in decreased angioenesis, vascular remodeling, inflammation, and increased clearance of lipoproteins • TFPI co-localizes with TF, regulating its effects within atherosclerotic lesions • TFPI also inhibits matrix metalloproteinases which play a pivotal role in destabilizing plaques • Studies have shown that TFPI-deficient mice have significantly more plaques than control mice and that overexpression of TFPI is associated with lower cholesterol levels and reduced plaque development
Anticoagulation Pathways in Vascular Inflammation: Protein C • Thrombin, despite its many procoagulant effects, also acts as an anticoagulant. It activates protein C by binding to protein C receptors. • Protein C then dissociates and forms a complex with protein S leading to inactivation of factors Va and VIIIa, therefore down-regulating additional generation of thrombin • Studies have indicated that atherosclerotic vessels have decreased protein C receptor expression, leading to decreased anticoagulant activity/regulation of thrombin
Conclusion • There is an intimate cross-linkage between hemostasis and inflammation in atherosclerosis • While anticoagulant therapy is important in prevention of thrombosis, it has not yet demonstrated regression of plaque growth • However, while long-term warfarin administration has not shown any visible effect on plaque progression, patients who under went CABG showed a 35% reduction in mortality 3 years after discontinuation. This evidence leads to the possibility of warfarin therapy to alter plaque phenotypes
Future Application • With traditonal vascular imaging using ultrasound, it has been difficult to accurately examine phenotypes and changes of plaques due to poor tissue penetration. • The use of high-resolution MRI in assessing plaque characteristics will support the phenotyping of vasculature walls as a method of determining the role of hemostasis in atherosclerosis • Currently, very few medications target relevant molecules of hemostasis. With this potential, new research and therapeutic options should be investigated • Oral direct inhibitors of Xa and thrombin • Small molecules that can access vessel walls and potentially alter plaques • DX-9065A • Pradaxa
References • Borissoff, Julian I., Henri M. Spronk, and Hugo Ten Cate. New England Journal of Medicine 2011; 364:1746-760. • Dipiro, Joseph T., Terry L. Schwinghammer, and Cecily V. Dipiro. “Venous Thromboembolism.” Pharmacotherapy Handbook. By Barbara G. Wells. 7th ed. New York: McGraw-Hill Companies, 2009. 163-65. • Katzung, Bertram G., Susan B. Masters, and Anthony J. Trevor. "Drugs Used in Disorders of Coagulation." Basic and Clinical Pharmacology. 11th ed. New York: McGraw-Hill Companies, 2009. 587-91