Download
1 / 16
160 likes | 208 Views
Explore the prevalence of ankylosing spondylitis, its burden, late diagnosis, and milestones in therapy. Discover the benefits of exercise, ASAS criteria, and outcomes in AS exercise studies. Learn about AS assessment, evidence-based studies, and ASAS/EULAR recommendations for non-pharmacological management.

E N D
Exercise in Ankylosing Spondylitis Prof. Pál Géher MD
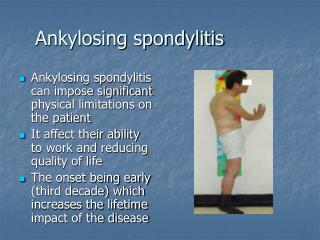
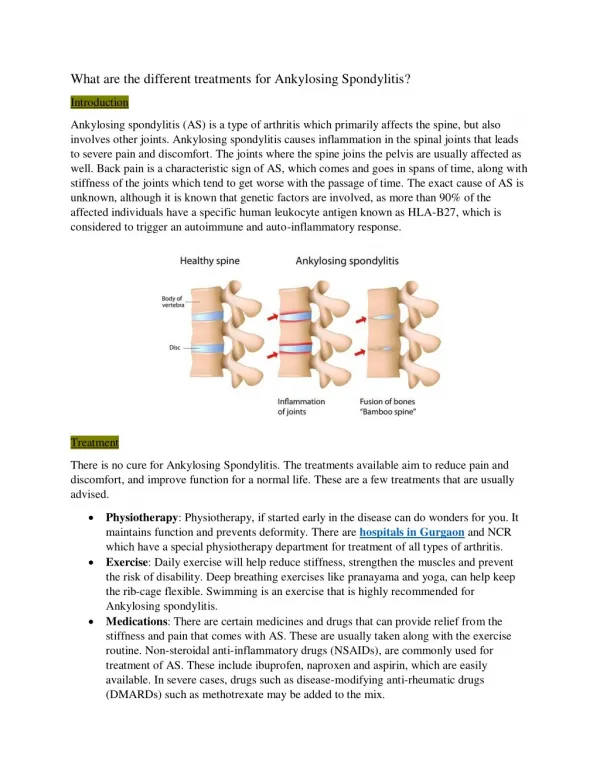
Ankylosing Spondylitis • Prevalence: 0.1% to 1.4%. • Significant burden of disease, similar to RA. • HLA B27 association. • Diagnosed late. • Underdiagnosed. • Unsatisfactory treatment.
Milestones of AS therapy • 1921. X-ray treatment. • 1949. Phenylbutazon. • 1965. Indometacinum. • ? Exercise • 2000. Biologics.
Studies on exercise in AS • Individual – conducted- exercise. • Group - conducted – exercise. • Individual exercise. No accepted protocol! 4. Underwater exercise – no study available.
ASAS 50 % response criteria At least 50% or in absolute value 10 mm(VAS 0-100 mm)improvement 3 domains: • Patient’s opinion • Pain • Function = BASFI • Inflammation = BASDAI 5.& 6.questions
Outcomes in exercise in AS • Function. • Pain. • Spinal mobility. • Stiffness. • Patient’s opinion.
Individual- conducted - exercise • 4 months, randomized, one center. • 26 treated, 27 controll. • Function - 23 % improvement. • Pain ? • Spinal mobility - 42 % improvement (finger-floor distance). • Stiffness ? • Patient’s opinion ? Kraag G et al: J Rheumatol 1994; 21: 261-3.
Group - conducted – exercise • 9 months, randomized, one center. • 6 weeks, individual-conducted- exercise, 68 patients individual exercise at home, once weekly group exercise,76 patients individual exercise at home. • Function - 32 % difference (4% improvement). • Pain ? • Spinal mobility - 7 % improvement (Schöber). • Stiffness ? • Patient’s opinion - 28 % improvement. Hidding A et al: Arthritis Care Res 1994; 7:90-6.
Evidence based studies • 3 trials, 241 patients. • Supervised vs. Individualised= supervised 50 % better (pain, stiffness) • Individual vs. None individual better. Dagfinrud H et al: The Cochrane Library, 2003.
ASAS/EULAR recommandations • 10 recommandations. • 3 general. • 5 pharma-therapy. • 1 surgery. • 1 non-pharmacological.
Non-pharmacological recommandation • Should include education, regular exercise and individual and group physical therapy….(level C) C= directly based on category III evidence or extrapolated recommendation from category I or II evidence.