Download
1 / 55
1.08k likes | 3.2k Views
Autoimmune Hemolytic Anemias. Donald R. Branch, Ph.D. Scientist Research & Development Canadian Blood Services Toronto, Ontario CANADA don.branch@utoronto.ca. Lecture Outline. Diagnosis of hemolytic anemias Immune hemolytic anemias Classification of AIHAs

E N D
Autoimmune Hemolytic Anemias Donald R. Branch, Ph.D. Scientist Research & Development Canadian Blood Services Toronto, Ontario CANADA don.branch@utoronto.ca
Lecture Outline • Diagnosis of hemolytic anemias • Immune hemolytic anemias • Classification of AIHAs • Serological diagnosis of specific AIHAs • Selection of blood for transfusing patients with AIHAs • Transfusion of patients with AIHAs
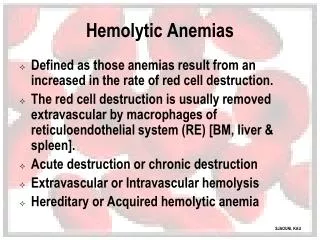
Diagnosis of Hemolytic Anemia • Shortened red cell survival (<100 days) • Structural, Hb variant, drug oxidant, immune • Can be acute (intravascular hemolysis) • Extravascular hemolysis • Can be life threatening What is Hemolytic Anemia?
Tests to Diagnose AIHA • Hemoglobin and hematocrit • Rule-out bleeding/hereditary causes – red cell morphology and blood film • Reticulocyte count • Bilirubin • Serum haptoglobin • LDH • Other tests (hemoglobinemia, hemosiderin) • DAT! • Cooperation between blood bank, hematology and urinalysis depts.
Immune Hemolytic Anemias DIRECT ANTIGLOBULIN TEST Test for IgG and/or complement coating the patient’s red blood cells
Classification of Immune Hemolytic Anemias • Alloimmune HTR DHTR HDFN • Autoimmune hemolytic anemias (AIHAs) DAT-positive DAT-negative • Drug-induced Autoimmune Drug-adsorption Immune-complex • Bystander Immune Cytolysis Sickle cell hemolytic transfusion reaction syndrome Reactive hemolysis
Classification of AIHAs Warm Antibody AIHA (warm AIHA) Cold Antibody AIHA (cold agglutinin syndrome; CAS) Paroxysmal Cold Hemoglobinuria (PCH) Combined Cold and Warm (“Mixed AIHA”) Atypical AIHA AIHA with a Negative DAT Warm Antibody AIHA Caused by IgM or IgA Autoantibodies Drug-Induced AIHA (drug-induced immune HA)
Warm Antibody AIHA and DAT • 70% of all AIHA are warm type • ~80% of warm AIHA prefer oldest RBCs • ~20% have no preference for age of RBCs • Associated with IgG, (IgA), (IgM) autoantibodies: DAT: IgG + C (67%) IgG only (20%) C only (13%) Must use a polyspecific antiglobulin reagent for DAT
Criteria for Diagnosis of Cold Antibody AIHA • Clinical findings indicative of acquired hemolytic anemia. • Positive direct antiglobulin test with anti-C3d ONLY! • Serum antibody optimally reactive at 4C but can react up to 30C, usually anti-I/i specificity
Criteria for Diagnosis of Mixed AIHA • Evidence indicative of acquired hemolytic anemia. • Severe hemolysis – intravascular/extravascular • DAT positive with BOTH IgG and C3d. • Serum contains an IgG antibody reactive at 37C indistinguishable from warm autoantibody. • Serum ALSO contains LOW TITER antibody reactive up to 30C (usually 37C) that is optimally reactive at 4C and is IgM; often shows anti-I/i. • Eluate contains IgG antibody having same specificity as serum antibody. • RESPONDS remarkably WELL to steroid therapy. (Shulman IA, Branch DR, et al. Autoimmune hemolytic anemia with both cold and warm autoantibodies. JAMA 253:1746-1748, 1985)
Paroxysmal Cold Hemoglobinuria (PCH) • Incidence: May be quite common in young children. • Acute onset of severe hemolysis with hemoglobinemia and hemoglobinuria. (hemoglobinuria very common). • Erythrophagocytosis by neutrophils is common and is distinctive. • Donath-Landsteiner test is diagnostic. • Patients have a stormy course but good ultimate prognosis.
Erythrophagocytosis in PCH RBC rosetting around neutrophils and erythrophagocytosis by neutrophils, rather than monocytes, are prominent findings in PCH. Rarely seen in other forms of immune hemolysis, where monocytes are usually involved. May be first clue to diagnosis.
The Donath-Landsteiner Test Characteristics of Typical D-L Antibodies Biphasic Hemolysin IgG Immunoglobulin Class Anti-P Specificity May also react by IAT
P p P + complement
DAT-negative AIHA • Rare • Often severe - fatal • Sometimes anti-IgA/anti-IgM useful • Mononuclear phagocyte assay may be useful – use patient monocytes • Often responds to steroid treatment
Criteria for Diagnosis of DAT-negative AIHA • Evidence indicative of acquired hemolytic anemia. • DAT negative with anti-IgG/anti-C3d • No unexpected antibodies detectable in serum or eluate (sometimes antibody can be detected in eluate) • Responds to prednisone treatment
Specificity of Warm Autoantibodies Not Usually Necessary – Academic Exercise • Anti-Rh-like specificity • Anti-e or anti-E (SIMPLE SPECIFICITY) • Anti-pdl – does not react with –D- or Rhnull • Anti-dl – does not react with Rhnull • Relative Rh specificity – titration studies • Type I or Type II Autoantibodies • Other blood groups – Kell, Gerbich (high frequency antigens)
A Guide to Transfusion of Patients with Autoimmune Hemolytic Anemia
Important Principles • Indications for transfusion are not significantly different than for similarly anemic patients without AIHA. • Specialized laboratory procedures are necessary. Critical to look for alloantibodies • Communication between laboratory personnel and clinicians is critical.
Risks of Transfusion in AIHA • Autoantibody will cause shortened survival of transfused RBC. • Alloantibodies may be present in addition to the autoantibody. Must Be Identified and Antigen-Negative Blood Given! • Risks caused by the increase in RBC mass as a result of transfusion.
Blood Transfusion in Autoimmune Hemolytic Anemia Blood should never be denied a patient with a justifiable need, even though the compatibility test may be strongly positive. Probably the most common mistake is reluctance to transfuse even those patients with severe anemia.
Communication Between Clinician and Transfusion Service Responsibilities of Transfusion Service • Initiate communication. • Indicate extent of compatibility testing performed, e.g., auto- or alloadsorption. • Clinician should be assured that, after appropriate compatibility testing, an acute HTR is unlikely. • Indicate that RBCs will provide temporary benefit even if they do not survive normally because of the patient’s autoantibody.
Communication Between Clinician and Transfusion Service Responsibilities of Clinician • Indicate urgency of situation. • Understand principles of compatibility testing. • Seek assurance that appropriate compatibility testing is to be performed.
Indications for Transfusion • A common mistake is reluctance to transfuse patients with AIHA. • If appropriate compatibility procedures are performed, survival of transfused RBCs is generally about as good as that of the patient’s own RBCs. Alloantibodies MUST be ruled out! • Significant temporary benefit is to be expected. • Patients should not be denied transfusion because of an RBC autoantibody.
ABO and Rh “Spontaneous” Agglutination IgG auto - Treat cells with ZZAP to remove autoantibody and retype IgM auto – warm everything to 37C and retype or ZZAP treat and retype (Branch DR, Petz LD. A new reagent (ZZAP) having multiple applications in immunohematology. Am J Clin Pathol. 78:161-167, 1982)
RBC ALLOANTIBODIES IN PATIENTS WITH WARM AUTOANTIBODIES • #ANTIBODIES/ % OF SERA • REFERENCE#SERA TESTEDWITH ALLOABS • Morel 8/20 40 • Branch and Petz 5/14 36 • Wallhermfechtel et al 19/125 15 • Laine and Beattie 41/109 38 • James et al 13/41 32 • Issitt et al (alloadsorptions) 13/34 38 • Issitt et al (autoadsorptions) 5/41 12 • Leger and Garratty 105/263 40 _______ • TOTALS:209/ 64732% • (Branch DR, Petz LD: Detecting alloantibodies in patients with autoantibodies. Transfusion 39:6-10, 1999) (editorial)
Adsorption Procedures • Warm autoadsorption using ZZAP is the optimal procedure for alloantibody detection. • One should obtain adequate volumes of patient’s RBCs to perform the procedure. • RBCs should be retained for subsequent procedures. • The number of ZZAP autoadsorptions needed is variable depending on the strength of the IAT and the ability to reduce the DAT. • Usually 2 adsorptions is sufficient • Autoadsorption is not reliable in a recently transfused patient.
Allogeneic Adsorption • If patient’s RBCs are not available for autoadsoprtion. • If the patient has been transfused recently, and if the patient’s pre-transfusion RBCs are not available for autoadsorption.
Selection of Red Cells for Allogeneic Adsorption • R1R1 • R2R2 • rr • One cell Jk(a-) • Another cell Jk(b-) • Use ZZAP to denature other important antigens
Allogeneic Adsorption • Advance planning is important ! • Large aliquots of appropriately phenotyped RBC should be obtained, treated with ZZAP, and stored at 4oC for up to 2 months. • If such procedures are infrequent, cryopreservation may be preferable. • Phenotyping patient may make it feasible to use fewer cells in adsorptions.