Download
1 / 37
390 likes | 1.21k Views
Interpretation of Chest Radiographs. UNC Emergency Medicine Medical Student Lecture Series. Objectives. The Basics Approach to interpretation Anatomy Interstital disease Alveolar disease Pattern Recognition Practice!. Interpretation. Use a systematic approach

E N D
Interpretation of Chest Radiographs UNC Emergency Medicine Medical Student Lecture Series
Objectives • The Basics • Approach to interpretation • Anatomy • Interstital disease • Alveolar disease • Pattern Recognition • Practice!
Interpretation • Use a systematic approach • Use or develop one you like • Use the same approach every time • Describe what you see • Form a differential based on patient presentation and appearance of x-ray • If you find an abnormality, don’t stop there • Finish your systematic reading • The second lesion is often missed
Systematic Approach • ABCDE • Airway (trachea) • Midline v. deviated or rotated, FB in trachea, ET tube position • Bones (clavices, ribs, humeri, etc) • Cardiomediastinal silhoutte • Diaphragms (and the costophrenic angles) • Everything Else (lung fields, soft tissues, tubes, lines, wires, devices, etc)
Anatomy Trachea Aortic knob Right main stem bronchus Left main stem bronchus Pulmonary artery Pulmonary artery Right atrium Left ventricle
Anatomy Upper lobes Middle lobe Lingula Right costophrenic angle Stomach Left hemidiaphragm Lower Lobes
Upper lobes Right middle lobe Lower lobes Lingula
Common Views PA/Lateral CXR PA Right anterior oblique Left Lateral AP Right lateral decubitus AP supine Portable CXR
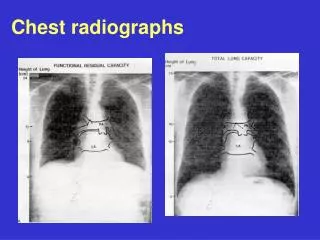
These are from the Same Patient Explain the difference…..
PA AP Always get a PA film to avoid cardiac magnification Exceptions: trauma, active cardiac chest pain, unstable, unable to cooperate with procedure
Silhouette Sign • Two substances of the same density, in direct contact, cannot be differentiated from each other on x-ray • Common locations • Lower lobes-diaphragms • Right heart border – RML • Left heart border – Lingula • Left diaphragm – Heart (on lateral view)
Air Bronchogram Sign • Visualization of air in the intrapulmonary bronchi • Abnormal • Denotes a pulmonary lesion/consolidation (excludes a pleural or mediastinal lesion) • Seen in pneumonia, pulmonary edema or pulmonary infarct Silhouette sign An air bronchogram within the heart shadow suggests LLL consolidation
Interstitial Lung Disease • The vessels (lung markings) appear more prominent • Alveoli are still aerated • DDx: Pulmonary edema, inflammation, tumor, fibrosis
Alveolar Disease • Vessels are less visible in the area of disease • Lung is not aerated • May have air bronchograms or silhouette sign • DDx: Bacterial pneumonia, pulmonary edema
Let’s Practice • What type of film • Describe what you see • Consolidation, infiltrate, nodular, diffuse, streaky, opacification • Look for Silhouette sign and air bronchograms • Is it an interstitial or alveolar pattern? • Other findings… • Give differential or diagnosis
Opacification of right hemithorax, obscured left hemidiaphram DDx: Massive pleural effusion, right pneumonectomy
Air-fluid (cavitary) lesion Opacification of left hemithorax, air-fluid level in left upper lobe, left clavicular fracture Diagnosis: Left empyema after trauma
Same patient Lateral view Air-fluid level
“Spine Sign” http://images.google.com/imgres?imgurl=http://www.residentandstaff.com/content/RSP/2006/07/img/Case_pneum_1.jpg&imgrefurl=http://www.residentandstaff.com/issues/articles/2006-07_02.asp&h=572&w=580&sz=72&hl=en&start=23&um=1&tbnid=wBsgta58mO7XPM:&tbnh=132&tbnw=134&prev=/images%3Fq%3Dleft%2Blower%2Blobe%2Batelectasis%26start%3D21%26ndsp%3D21%26um%3D1%26hl%3Den%26sa%3DN
Dx: Subcutaneous air in neck and shoulder and pneumomediastinum (left heart border)
Lack of lung markings on right, collapsed lung Dx: Complete right pneumothorax Is it a tension pneumothorax? Collapsed lung
NO! • Tension Pneumothorax • Mediastinum is shifted to opposite site of pneumothorax • Look at trachea and bronchi • Look at heart • Your patient is unstable or in distress • Absent breath sounds • Respiratory difficulty, hypoxia • Hypotension • Trachea shifted
Thank You! Any Questions?