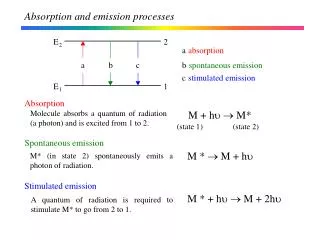
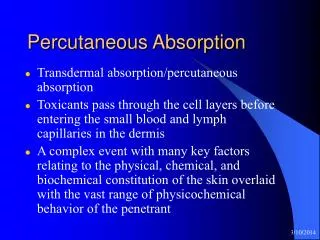
Percutaneous Absorption
Percutaneous Absorption. Transdermal absorption/percutaneous absorption Toxicants pass through the cell layers before entering the small blood and lymph capillaries in the dermis

Percutaneous Absorption
E N D
Presentation Transcript
Percutaneous Absorption • Transdermal absorption/percutaneous absorption • Toxicants pass through the cell layers before entering the small blood and lymph capillaries in the dermis • A complex event with many key factors relating to the physical, chemical, and biochemical constitution of the skin overlaid with the vast range of physicochemical behavior of the penetrant
Transdermal control • Local or systemic pharmacological response using dermally applied drugs • Current research is divided • restraint (slow release technology) and • enhancement (occlusion, permeation enhancers)
Toxicological hazard • Accidental or deliberate (chemical warfare) • commercial and home and garden pesticides • polymer and paint chemicals • detergents and cleaning chemicals • a broad range of heavy industrial chemicals • unscheduled exposures to environmental accidents and • mishandling of toxic waste disposal
Percutaneous Absorption • With the exemption of highly volatile chemicals, the principal organ exposed to these hazards is skin • Research in this area is directed towards understanding transdermal flux rates and the toxicological consequences of penetration • At the practical end, such data contribute to risk assessment
1. Factors Affecting Percutaneous Absorption • Biological factors • skin age • skin condition • anatomical site • skin metabolism • circulatory effects
1. Factors Affecting Percutaneous Absorption • Physicochemical factors • hydration • drug-skin binding • temperature
1. Factors Affecting Percutaneous Absorption • Physical factors • drug concentration • surface area • exposure time • occlusion • vehicle
2. Mechanisms of Percutaneous Absorption • Mechanisms by which chemicals cause visible effects on the skin differ from chemical to chemical • disruption of lipids and membranes • protein denaturation • keratolysis • cytotoxicity
2. Mechanisms of Percutaneous Absorption • The rate-determining barrier is Stratum Corneum (nonviable epidermis), which is densely packed keratinized cells (nuclei lost, biologically inactive) • SC contains 75-80% lipophilic materials • very little triglycerids (0%) • cholesterol (27%) • cholesterol esters (10%) • various ceramides (41%; amides and/or esters of saturated and unsaturated fatty acids)
Figure 5. The sequential steps involved in percutaneous absorption 1. Partitioning 2. Diffusion 3. Partitioning 4. Diffusion 5. Capillary uptake Mukhtar, H., 1992. Pharmacology of the Skin. CRC Press, Inc., Boca Raton, FL.
Figure 6. The putative pathways of penetration across the Stratum Corneum Mukhtar, H., 1992. Pharmacology of the Skin. CRC Press, Inc., Boca Raton, FL.
2. Mechanisms of Percutaneous Absorption • Appendageal transport makes a negligible contribution to the overall percutaneous flux across human skin. • however, transport through the appendageal route has been shown to be significant during the initial (non-steady-state) period of percutaneous absorption • Appendageal transport remains controversial • resent research has again raised the question of the participation of the hair follicles in percutaneous absorption
2. Mechanisms of Percutaneous Absorption • Permeation pathways • Polar (hydrophilic) • Path through corneocytes with their desmosomal connections • Nonpolar (lipophilic) • Agents dissolve in and diffuse through the lipid matrix between the protein filaments • Regional variations in skin permeability are correlated with quantitative differences in lipid content rather than SC thickness or cell number
3. Percutaneous Transport • Molecules traverse membranes either by • passive diffusion • solute flux is linearly dependent on the solute concentration gradient • active transport • typically involves a saturable mechanism • Percutaneous flux is directly proportional to the concentration gradient and, therefore, transport across the skin occurs primarily by passive diffusion
3. Percutaneous Transport • At steady state, the flux due to passive diffusion may be described by Fick’s 1st law J = kpa • J = flux of the permeant (moles/cm2s) • kp = permeability coefficient of the permeant through the membrane (cm/s) • ∆a = activity gradient across the membrane (moles/cm3)
3. Percutaneous Transport • kp is the inverse of the “resistance”, which the membrane offers to solute transport, and is defined by kp = KD / h • K = membrane-aqueous phase partition coefficient of the solute • D = diffusion coefficient of the solute in the membrane (cm2/s) • h = diffusion path length through the membrane
3. Percutaneous Transport • The flux rate is a rate process rate = (driving force) / (resistance) • The driving force for diffusion is the activity gradient (concentration gradient across the permeability barrier) • Molecular flux across the membrane can be determined by the solute’s size and lipophilicity if the driving force remains the same • Octanol/Water partition coefficient (Ko/w) has been chosen to be used as the index of lipophilicity
Laboratory Human Volunteer Study 1.0 ml of jet fuel is applied at two sites Exposure study was done inside a fume-hood to prevent inhalation exposure Surface area of exposure is 20 cm2 Tenax® tubes were used to measure evaporation from arm
Study Population • 5 male and 5 female adult volunteers • Breathing-zone, dermal tape-strip, breath, urine, and blood samples • Exclusion criteria • occupational exposure to chemicals in JP-8 (e.g., auto mechanics) • cardiovascular disease • atopic dermatitis • smoking • use of prescription medication for illness • alcohol consumption during the study
How to estimate permeation of JP-8 components across the skin Fick’s Law of Diffusion L1 x0, C(x0) L2 J = -D x1, C(x1) Permeability Coefficient Kp (cm/h)
Human Skin Permeability Coefficients (x 10-5) Rat Kp from McDougal et al. (2000)
Estimation of the Internal Dose hands ≈ 840 cm2 3 mg/ml 1 hr M = Kp CJP-8 A t rat, pig, human 4 Mrat = 1.29 mg Mpig = 0.53 mg Mhuman = 0.13 mg 10 Rat Kp from McDougal et al. (2000) Pig Kp from Muhammad et al. (2004)
Metabolism of Xenobiotics • Most foreign compounds are lipophilic and able to penetrate lipid membranes and to be transported by lipoproteins in the blood • These lipophilic compounds are substrates for biotransforming enzymes • Epidermis is the major site in the skin for metabolism of xenobiotics, steroids, and vitamins
Metabolism of Xenobiotics • After invasion, the xenobiotic substance is first chemically activated (usually by oxidation) • phase I metabolic reaction, where a polar reactive group is introduced into the molecule, rendering it a suitable substrate for phase II metabolism • cytochrome P-450 isoenzymes • localized mainly in the endoplasmic reticulum (microsomal fraction) • activities about 1-5% of those in the liver • Pre-carcinogenic chemicals can be converted to carcinogenic metabolites
Marzulli, F.N. and Maibach, H.I., 1996. Dermatotoxicology, 5th ed. Taylor & Francis, Washington, DC.
Transferases, Epoxyhydrase, NQR P-450 Drug Or Xenobiotic Active Xenobiotic (e.g., epoxides) Elimination Binding to Macromolecules (e.g., membranes, proteins, DNA, RNA) Chemocarcinogenesis, Mutagenesis, Teratogenesis, Sensitization Figure 7. Schematic of metabolism of xenobiotics Marzulli, F.N. and Maibach, H.I., 1996. Dermatotoxicology, 5th ed. Taylor & Francis, Washington, DC.
Metabolism of Xenobiotics • Activated metabolite is transformed by phase II enzymes (transferases, reductases) • all major transferases are found in the skin (about 10% of hepatic activities) • NAD(P)H-quinone reductase (NQR) • epoxide hydrolase • Formation of highly hydrophilic metabolites, which are more readily excreted (e.g., mercapturic acids)
Metabolism of Xenobiotics • Some foreign compounds (e.g., electrophiles that undergo nuclear substitution) are not transformed by phase I enzymes but react directly at the site of contact; ultimately eliminated by phase II enzymes • e.g., mono- and multifunctional acrylates • Skin metabolizing enzymes differ both quantitatively and qualitatively from those in the liver, particularly by their relative proportions, composition, and interactions