Case Presentation:
More than just a left leg Deep Vein Thrombus!. Majidah Bukhari MD , Rami Abdelshaheed MD , Alex C Spyropoulos, MD, FACP, FCCP, FRCP Ally P. H. Prebtani MD, FRCPC Department of Internal Medicine, McMaster University, Hamilton, Canada. ABSTRACT. Case Presentation:. Pathophysiology.

Case Presentation:
E N D
Presentation Transcript
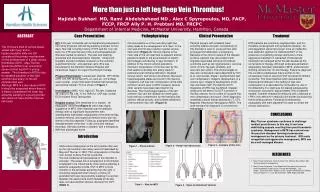
More than just a left leg Deep Vein Thrombus! Majidah Bukhari MD, Rami Abdelshaheed MD ,Alex C Spyropoulos, MD, FACP, FCCP, FRCP Ally P. H. Prebtani MD, FRCPC Department of Internal Medicine, McMaster University, Hamilton, Canada ABSTRACT Case Presentation: Pathophysiology Clinical Presentation Treatment HPI: A 30 year old female with endometriosis presented to her family physician with left leg swelling and pain for two days. She had no family history of VTE and her only risk factor for VTE was the use of the oral contraceptive pill. She was started on warfarin. The pain and swelling worsened and she presented to Hospital. Ultrasound Dopplers showed complete occlusion of the common, superficial femoral, and popliteal veins. She was transferred to the Hamilton General Hospital with intravenous heparin for urgent thrombolytic therapy. Physical Examination: Looked well, afebrile. BP 125/66, a HR 107, RR 18 O2 Sat 97% on room air. CV & Resp exam normal. Lower limb exam showed that the left leg was entirely swollen. This is shown in Figure 1 Investigation: WBC 10.5, Hgb 127, Plt 249, Creatinine 49, urea 2.4, Na 138, K 4.0. INR 2.2. CXR was normal. ECG showed Sinus Tachycardia Hospital course: She remained on iv heparin. An angiogram performed(Figure 2) which was highly suggestive of MTS. She received local thrombolytic therapy with no significant improvement then subsequently had balloon angioplasty of the external iliac, common femoral, and superficial femoral veins with two stents in the iliac segment. Follow up angiogram identified reestablishment of the flow in the veins with residual thrombus. She was started on warfarin with a therapeutic INR then discharged home. Patients present with unilateral lower extremity edema and pain. A propensity for this disorder is seen in young women after prolonged immobilization or pregnancy. Because of the chronic nature of the disease process, patients may also present with stigmata associated with post-thrombotic syndrome such as skin pigmentation, varicose veins, chronic leg pain, phlebitis, and recurrent skin ulcers. The clinical stages of iliac vein compression were described by Kim et al, and include: Stage I, asymptomatic iliac vein compression; Stage II, development of a venous spur; Stage III, development of left iliac vein Deen Vein Thrombosis (DVT). Diagnosis of MTS may be difficult. Doppler ultrasound will detect if a DVT is present in the iliac vessels, but is unable to visualize iliac vein compression and spurs. Other diagnostic modalities include helical abdominal CT, CTV, Magnetic Resonance Venography (MRV). The gold standard for diagnosis is conventional venography. MTS patients are commonly asymptomatic, and it is therefore unrecognized until symptoms develop . As anticoagulation alone has proven to be an ineffective sole treatment regimen for iliofemoral DVT in the presence of underlying venous obstruction, more aggressive treatment is warranted. Endovascular treatment has emerged within the last decade as the cornerstone of therapy. Although endovascular balloon angioplasty has been attempted in MTS, endovascular stenting remains the 1st-line therapy. Failure to diagnosis this condition predisposes these women to the unnecessary risks of recurrent DVT and post-thrombotic syndrome. The initial treatment with documented iliofemoral thrombosis in the setting of iliac vein compression is to decrease the clot burden by use of thrombectomy. If a stent was not placed subsequently, reocclusion occurred in approximately 70% of patients treated. Catheter-directed thrombolysis with urokinase or t-PA is very effective in reducing clot burden by dissolving the thrombus present. Following thrombectomy, angioplasty with stent placement is used to correct the venous obstruction. Chronic pulsations of the overriding right iliac artery leads to the development of a “spur” in the vein wall and this spur results in partial venous obstruction (Figure 2). Chronic trauma to the inner side of the vein wall due to adjacent arterial pulsations leads to the accumulation of elastin and collagen contributing to spur formation. In addition to the chronic arterial pulsations, mechanic compression of the iliac vein by the thick-walled overriding iliac artery leads to extensive local intimal proliferation, impaired venous return, and venous thrombosis. Moreover, hypercoaguable states are found in the majority of patients. Left iliac vein compression is the most common variant seen in MTS; however, several other variants have been described in the literature. The morphologic features of the left common iliac vein are dividedinto three types: focal extrinsic compression by the overlyingiliac arteries, diffuse atrophy, and cordlike obliteration of left common iliac vein. (Figure 4) The Virchow’s triad of venous stasis, vessel wall injury, and a hypercoagulable state are still considered the primary mechanisms for the development of a deep venous thrombosis (DVT). May-Thurner Syndrome (MTS) is an uncommon cause of a left leg DVT in young women. The thrombus in MTS is due to repeated pulsation of the right common iliac artery on the left common iliac vein. Although MTS is a rare cause of DVT, it should be suspected where there is a history of persistent left lower leg extremity swelling in a young woman who does not have another obvious risk factor. CONCLUSIONS May-Thurner syndrome continues to challenge medical practitioners to this day. It can have debilitating sequela resulting from post-thrombotic syndrome. Management of MTS has evolved over the past few decades favoring endovascular management as the primary treatment. With early recognition and aggressive management, MTS can be a well-managed disease. Introduction Obstructive compression of the left common iliac vein by the right common iliac artery was first described by May and Thurner in 1957. This compression of the iliac vein, known as May-Thurner syndrome. The true incidence and prevalence of this disorder is unknown. The actual risk of progression to thrombosis is believed to be influenced by other factors affecting a patient's coagulation profile. DVT in MTS is more common in the left lower extremity than the right. It should be suspected when there is a history of persistent left lower leg extremity swelling in a woman between the second and fourth decade of life who does not have another obvious risk factor for DVT. (Table 1) Figure 3 – Anatomy of Iliac Vein Figure 2 – Partial Vein Obstruction Figure 1 – Physical Exam REFERENCES • May-Thurner Syndrome: Omar Al-Nouri, DO, MS and Ross Milner, MD. Vascular disease management. • May-Thurner Syndrome: Case Report and Review of the Literature Involving Modern Endovascular Therapy Neil Moudgill*, Eric Hager, Carin Gonsalves, Robert Larson, Joseph Lombardi,Paul DiMuzio. Vascular Volume 17, Issue 06, December 2009, Pages 330-335. Table 1 – Risk for MTS Figure 4 – Types of Anatomical Variants