Download
1 / 102
1.02k likes | 1.7k Views
Explore the importance of mobility and Range of Motion exercises to maintain joint flexibility and prevent muscle deterioration. Learn the principles, key factors, types of ROM, and proper techniques for assisted and active ROM exercises.

E N D
Mobility • Mobility refers to a person’s ability to move about freely. • Immobility refers to a person’s inability to move about freely. • Mobility & immobility are the endpoints of a continuum with many degrees of partial immobility in between. mobility immobility Some clients move back and forth, some clients remain absolute.
Ability to Move • The ability to move & function is a function most people take for granted. • The level of mobility has a significant impact on an ind.’s physiological, psychosocial, & developmental well-being (Hamilton & Lyon, 1995). • When there is an alteration in mobility, many body systems are at risk for impairment. • Cardiovascular functioning – orthostatic hypotension • Pulmonary complications – pneumonia • Promote skin breakdown, muscle atrophy etc • Such changes can lead to altered self-concept & lowered self-esteem.
Medical Conditions that can Alter Mobility • Fractures/sprains • Neurological conditions – spinal cord injury, head injury • Degenerative neurological conditions – Myasthenia gravis, Huntington’s chorea
Range of Motion(ROM) • definition: • exercising joints through the available motion to maintain available range and flexibility of joint structures
Purpose of ROM • maintain joint movement and integrity • preventdeterioration of joint structures, ankylosis and contractures
Indications for ROM • patients on prolonged bed rest • prevention of contracture • stimulates circulation
Types of ROM • active (AROM) • performed by patient • patient moves the joints through available ROM • maintains muscle strength and joint mobility
Types of ROM • active assistive (AAROM) • performed by patient with assistance from another person or mechanical device • patient uses stronger limb to move or support weaker limb • practitioner completes movement through full available ROM
Types of ROM • passive (PROM) • performed for patient by healthcare worker or caregiver • moves all muscle groups within each plane over each joint • does not maintain muscle strength • maintains joint flexibility & integrity • Why would this be done?
Types of ROM • stretching • forcing movement beyond the available ROM • contraindicated for most healthcare personnel
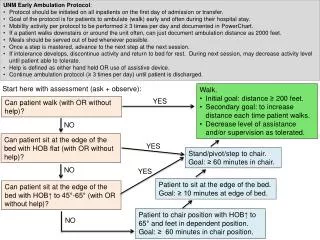
Principles of ROM • Check doctor’s orders • Know the patient diagnosis and rationale for ROM • Explain the procedure to the patient
Principles of ROM • use good body mechanics • expose limb being exercised • support body part proximal to joint • use slow smooth rhythmic motion
Key Factors for ROM • start ROM exercises on the unaffected side • start each movement in neutral position • use a firm comfortable grip while maintaining support of the extremity • avoid forcing beyond range • avoid overexerting patient • avoid skin friction • exercise just below point of pain, NOT beyond
Key FactorsforROM • if rigidity occurs slightly decrease ROM until it subsides • stop if spastic contraction occurs • talk to patient to help them relax • expect heart rate and respirations to rise • exercise 2-3x’s daily, 5-10 movements(see physician’s or Physical Therapist orders) • document procedure & patient reaction
Perform Exercises in Head to Toe Format • Start with the head and move down, always do bilaterally • Do not grasp the joint directly • Cup the joint gently (prevents pressure) • Do not grasp fingernail or toenail • Important joints – thumb, hip, knee, ankle • Return to correct anatomic position • Move joint through movement 5 times/session
Example of Flexion • Elbow flexion • bend
Example of Flexion • Knee flexion • bend
Example of Flexion • Toes flexion • bend
Example of Extension • Knee extension • straight
Example of Extension • Head & Neck extension • straight
Example of Abduction • Hip abduction • away from midline of body
Example of Adduction • Toes adduction • toward midline
Examples of Rotation • Head and Neck rotation • turning part on its axis Left Right
Example of Rotation • Hip internal rotation • pivoting inward
Example of Horizontal Adduction • Shoulder horizontal adduction • toward body in transverse plane
Example of Supination • Forearm supination • rotate forearm, palm up
Example of Pronation • Forearm pronation • rotate forearm, palm down
Example of Opposition • Thumb opposition • oppose thumb tip base of little finger orto finger tip of each individual finger
Example of Eversion • Ankle eversion • sole of foot turned outward at the ankle
Example of Inversion • Ankle inversion • sole of foot turned inward at the ankle
Example of Dorsiflexion • Ankle dorsiflexion • an upward or backward motion of the ankle toward the hips
Example of Plantar Flexion • Ankle plantarflexion • a toe down motion of the foot at the ankle
Types of ROM exercises • Active – exercises the client is able to perform independently. • Passive – exercises performed for the client by someone else. • Active assisted – performed by a client with some assistance – client can move a limb partially through its ROM, but needs help completing the ROM.
Isometric/Isotonic Exercises • In addition to ROM exercises, some immobilized clients may be able to perform muscle-strengthening exercises. • Isotonic – cause muscle contraction & change in muscle length – walking, aerobics, moving arms & legs against light resistance. • Isometric – tightening or tensing of muscles without moving body parts. This increases muscle tension but do not change the length of muscle fibers. Isometric exercises are easily performed by an immobilized patient in bed. • Isotonic and isometric exercises help to prevent muscular atrophy and combat osteoporosis.
MMT • Manual Muscle Testing • Done to evaluate the individual strength and function of a muscle or muscle group • Done by therapist • https://www.youtube.com/watch?v=WTe175iGqVo
Goniometry • https://www.youtube.com/watch?v=kTp4vfxjRWc • Stationary arm : placed parallel with the longitudinal axis of the fixed part • Movable arm : along the longitudinal axis of the movable segment • Axis of rotation(pin) : at the intersection of the stationary & movable arms
Goniometry procedure • position joint in zero position and stabilize proximal joint component • move joint to end of range of motion (to assess quality of movement) • determine end-feel at point where measurement will be taken ( at end of available range of motion) • identify and palpate bony landmarks • align goniometer with bony landmarks while holding joint at end of range • read the goniometer • record measurement (e.g. elbow flexion = 130o)
Upper Ext. Test Position • Subject supine • Flatten lumbar spine (flex knees) • Shoulder no abduction, adduction or rotation • (note: to measure gleno-humeral motion, stabilize scapula) Shoulder flexion (0~180°) Goniometer Alignment • Axis – center of humeral head near acromion process • Stationary arm – parallel mid-axillary line • Moving arm – aligned with midline of humerus (lateral epicondyle)
Shoulder extension (0~60°) Test Position • Subject prone • Shoulder no abduction, adduction or rotation • (note: to measure gleno-humeral motion, stabilize scapula) Goniometer Alignment • Axis – center of humeral head near acromion process • Stationary arm – parallel mid-axillary line • Moving arm – aligned with midline of humerus (lateral epicondyle)
Shoulder abduction (0~180°) Test Position • Subject supine • Shoulder 0° flexion and extension • Shoulder laterally (externally) rotated • Shoulder abducted • Stabilize thorax (note: to measure gleno-humeral motion, stabilize scapula)
Shoulder abduction (0~180°) Goniometer Alignment • Axis – center of humeral head near acromion process • Stationary arm – parallel to sternum • Moving arm – aligned with midline of humerus



![[Insert exercise name]](https://cdn0.slideserve.com/1400721/insert-exercise-name-dt.jpg)