Download
1 / 20
210 likes | 457 Views
Transmissible Spongiform Encephalopathies. Prion Diseases. Classification of TSEs. Characteristic features of TSEs. Long asymptomatic incubation period (years) Fatal neurodegenerative disease Characteristic pathological changes in the brain (vacuoles).

E N D
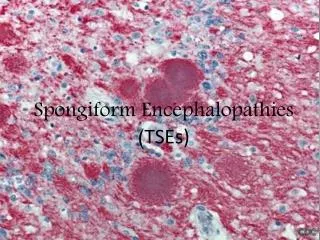
Transmissible Spongiform Encephalopathies Prion Diseases
Characteristic features of TSEs • Long asymptomatic incubation period (years) • Fatal neurodegenerative disease • Characteristic pathological changes in the brain (vacuoles) Neuronal degeneration & loss by apoptosis Astrocytic hypertrophy/ hyperplasia & microglial activation
Clinical signs • Pruritus – (scrapie) • Behavioural changes - nervousness/excitability - aggression • Ataxia/changes in gait • Weight loss (normal appetite) • Disturbances in body homeostasis • Excessive salivation (CWD) • Other (less common) – defective vision, fits etc.
Causative agent Originally designated “slow virus” diseases – infectious particles could pass through filters that exclude bacteria However, TSE agents showed several unusual features: - No detectable immune response - Extreme resistance to chemical/physical inactivation e.g. formalin, heat - Survives ionising and ultraviolet radiation capable of destroying nucleic acid - Not inactivated by proteases or denaturants
Protein-Only hypothesis Protein could be the infectious agent, inducing its own replication by causing conformational change of normal cellular PrPC into PrPSc PrPC PrPSc Prion = proteinaceous infectious particle (of “virion”)
Prion hypothesis • Protease resistant protein (PrP = prion protein) co-purifies with infectivity • Gene encoding PrP is part of the host genome Alternative hypothesis: “Virino” – TSE agent is an informational hybrid of an independent genome (nucleic acid) and one or more host genes (host-encoded protein, PrP)
Detection/strain typing of TSE agents - bioassay Scoring of affected brain areas Incubation period 1-2 years Remove brain (+ other tissues) at post mortem Inject tissue extracts into mice Recent development of cell culture methods – not in widespread use
Mr (K) 1 2 3 4 30 22 More rapid methods of PrPSc detection & strain typing Neuropathology Immunohistochemistry Western blot Sandwich immunoassay Most rely on proteinase K digestion to distinguish PrPSc from PrPC
Role of the immune system in peripheral pathogenesis • Scrapie (and other TSE agents) replicate in lymphoid tissues • Minimal pathology associated with lymphoid infection • No immune response (tolerance) • Immunodeficient animals are relatively resistant to disease
Role of the immune system in pathogenesis of TSEs Lymph node • Follicular dendritic cells (FDC) – important role in TSE replication • B cells – indirect role in maintaining FDC network • Dendritic cells – transport of infection/processing PrPSc? • Macrophages – clearance of infection/PrPSc? Dark zone Macrophage Germinal centre B cells Light zone FDC T cell zone T cells Dendritic cell
Peripheral pathogenesis of BSE Ingestion of BSE agent Tonsil Peyer’s patch Enteric nervous system Peripheral nerves? Vagus n Splanchnic n Central nervous system
Neuroinvasion • Via blood – evidence of early PrPSc deposition in circumventricular organs of brain • Via peripheral nerves (autonomic nervous system) – supported by evidence from sequential necropsies and transgenic mouse models
Meat products(?) BSE ? ? Scrapie vCJD ? ? Origin of BSE and routes of transmission
Transmission of scrapie Meat (intermediate host?) Foetus Placenta Saliva? Nasopharyngeal secretions Faeces Urine? Semen Blood (vector?) Milk
Natural transmission of scrapie • Vertical (maternal) transmission – in utero or perinatal (placenta/milk) • Lateral transmission – direct contact and/or environmental contamination? (placenta/blood/urine/saliva; evidence for persistence of infectious agent in soil) • Role of vectors? – hay mites, fly larvae – not substantiated
Transmission of BSE in cattle • No evidence for lateral transmission • No infectivity detected in blood/urine/milk • Maternal transmission – probably a rare occurrence • Epidemiological evidence supports extended common source epidemic i.e. feed containing infected meat and bone meal
Transmission of TSEs by blood transfusion • BSE and scrapie can be readily transmitted between sheep by blood transfusion • Follow up of 66 recipients of blood from donors who developed vCJD, has so far identified 4 individuals who probably acquired infection as a result of transfusion
Control of scrapie by selective breeding • • Aims to increase the frequency of resistant breeds • • Classifies sheep into 5 types based on PrP genotype • 1 most resistant • 5 most susceptible • ● Recommends that sheep of type 4 and 5 are not used for breeding • Banning feed that contains infected meat and bone meal
Control of BSE Number of confirmed cases Year 1st feed ban (ruminants) 2nd feed ban (all livestock) Active surveillance (EU)