ENDOCRINE SURGERY
ENDOCRINE SURGERY. Li, Henry Winston Li, Kingbherly Lichauco, Rafael Lim, Imee Loren Lim, Jason Morven Lim, John Harold. CASE. 20 years old, female Chief Complaint: RECURRENT LUMBAR PAINS. PHYSICAL EXAMINATION. Vital Signs BP:120/70 RR: 20/min PR: 70/min Neck

ENDOCRINE SURGERY
E N D
Presentation Transcript
ENDOCRINE SURGERY Li, Henry Winston Li, Kingbherly Lichauco, Rafael Lim, Imee Loren Lim, Jason Morven Lim, John Harold
CASE • 20 years old, female • Chief Complaint: RECURRENT LUMBAR PAINS
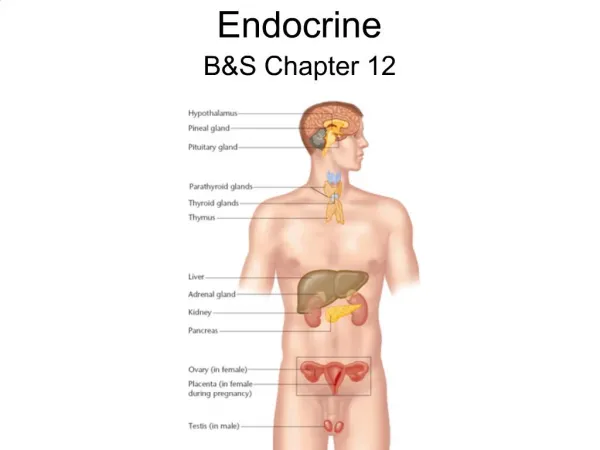
PHYSICAL EXAMINATION • Vital Signs BP:120/70 RR: 20/min PR: 70/min • Neck 2 x 2cm firm palpable mass within the right lobe of the thyroid which moves with deglutition; no other palpable masses • Chest (normal) • Abdomen Flat, normoactive bowel sounds, liver is not enlarged, no splenomegaly, (+) CVA tenderness
ANCILLARY PROCEDURES • Urinalysis: (+) red blood cells and crystals • IVP: (+) bilateral kidney stone
Salient Features • 20 year old female • Recurrent lumbar pains • Bilateral kidneys stones • RBC and crystals in urine • 2 x2 cm palpable mass within the right lobe of the thyroid with no other palpable mass • Costovertebral angle tenderness • No hepatomegaly, no splenomegaly
1. What further workups would you request? Justify • Serum tumor markers • Screen for pheochromocytoma • Screen for hyperparathyroidism
Serum tumor markers • Calcitonin: • produced by C-cells, an antihypercalcemic hormone which inhibits osteoclast-mediated bone resorption; • minimal role in calcium regulation • >10 pg/mL = diagnostic of MTC • CEA • Not specific for MTC • Also seen in colon CA and metastasis to the liver
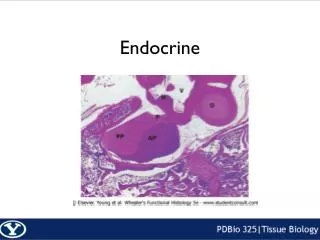
FNAC Examination Fragment of granular and amyloid material
CT Scan or MRI (chest/abdomen) • Procedures detect distant metastases especially if there is a very high level of calcitonin • Imaging studies requested only if there is suspected invasion
Screening for pheochromocytoma • 24h urine cathecholamines and metanephrines • Treated preoperatively
Determination of serum calcium levels, ionize calcium and parathyroid hormone level • 24 hour urinary calcium to differnetiate from BFHH • X-ray of spine and abdomen • Fine needle biopsy of the mass in the right lobe of the thyroid
Technetium-99m (99mTc) sestamibi scan • Salivary glands • Thyroid glands • Palpable mass
Technetium-99m Sestamibi Scan • Sestamibi: small protein which is labeled with the radio-pharmaceutical technetium-99 • Radioactive agent is injected into the veins of a patient with parathyroid disease • Radionuclide is concentrated in thyroid and parathyroid tissue but usually washes out of normal thyroid tissue in under an hour. It persists in abnormal parathyroid tissue.
Technetium-99m Sestamibi • After 1-2 hours, radioactivity in suspected parathyroid adenoma should persist.
Technetium-99m (99mTc) sestamibi radionuclide scan • Not used to confirm diagnosis of PHPT • Used to identify the location of the offending gland • > 80% sensitivity for parathyroid adenoma • Generally complemented with neck ultrasound which has 77% sensitivity
3. What is your clinical diagnosis? Basis? • Medullary thyroid carcinoma with concurrent primary hyperparathyroidism • BASIS: MTC- 2 x2 cm palpable mass within the right lobe , FNAC examination revealed granular amyloid material; PHPT- bilateral urolithiasis, elevated PTH and calcium assay
Medullary thyroid CA • 5% of thyroid malignancies and arise from the parafollicular or C cells of the thyroid • Forms: Sporadic (80%) hereditary (20%)- autosomal dominant inheritance, mutation of RET proto-oncogene
Primary Hyperparathyroidism • Increased parathyroid proliferation and PTH secretion independent of calcium levels • Affects females more than male • Sporadic type more common • Etiology -Parathyroid adenoma (80%) -Multiple adenoma or hyperplasia (15-20%) -Parathyroid CA (1%)
4. How would you manage this patient? Explain. • Manage the symptomatic disease (Medullary thyroid cancer and primary hyperparathyroidism)
Management for MTC • Total thyroidectomy -treatment of choice due to high incidence of multicentricity -bilateral central neck node dissection should be routinely performed due to frequent involvement of the central compartment nodes -patients with tumors larger than 1.5 cm should undergo ipsilateral prophylactic modified radical neck dissection, because greater than 60% of these patients have nodal metastases
Follow-up • Calcitonin and CEA 2-3 months post-op • If calcitonin >100, evaluate for residual neck disease or +/- distant metastasis • MEN IIA and MEN IIB: annual screen for pheochromocytoma
Prognosis • 10-year survival rate is approximately 80% • decreases to 45% in patients with lymph node involvement. • worst (35% at 10 years) in patients with MEN2B
Management for PHPT • PARATHYOIDECTOMY Indications - Markedly increased serum calcium - Episode of life threatening hypercalcemia episode - Reduced creatinine clearance - Kidney stones - Markedly elevated 24 hr urinary Ca excretion - Substantially decreased bone mass - Age: < 50 years old
Management for PHPT • In patients who have hypercalcemia at the time of thyroidectomy, only obviously enlarged parathyroid glands should be removed. • The other parathyroid glands should be preserved