Download

1 / 64
640 likes | 802 Views
بيش از يك ميليــــارد نفر در دنيااضافه وزن دارند 000/500 نفر د رآمريكا و اروپاي مركزي سالانه دراثر چاقي دچار مرگ زودرس ميشوند. در كشور ما بيش از 50 درصد بالغين اضافه وزن مشاهده ميشود باعث افزايش فشارخون ، بالارفتن سطح كلسترول خون و افزايش مقاومت درمقابل انسولين ميشود.

E N D
بيش از يك ميليــــارد نفر در دنيااضافه وزن دارند 000/500 نفر درآمريكا و اروپاي مركزي سالانه دراثر چاقي دچار مرگ زودرس ميشوند. در كشور ما بيش از 50 درصد بالغين اضافه وزن مشاهده ميشود باعث افزايش فشارخون ، بالارفتن سطح كلسترول خون و افزايش مقاومت درمقابل انسولين ميشود. درمطالعهاي در تهران درافراد 20 سال به بالا حدود 29 % زنان و 40% مردان وزن طبيعي دارند ولي از 40 سال به بالا دو سوم مردان و چهار پنجم زنان دچار اضافه وزن و چاقي هستند.
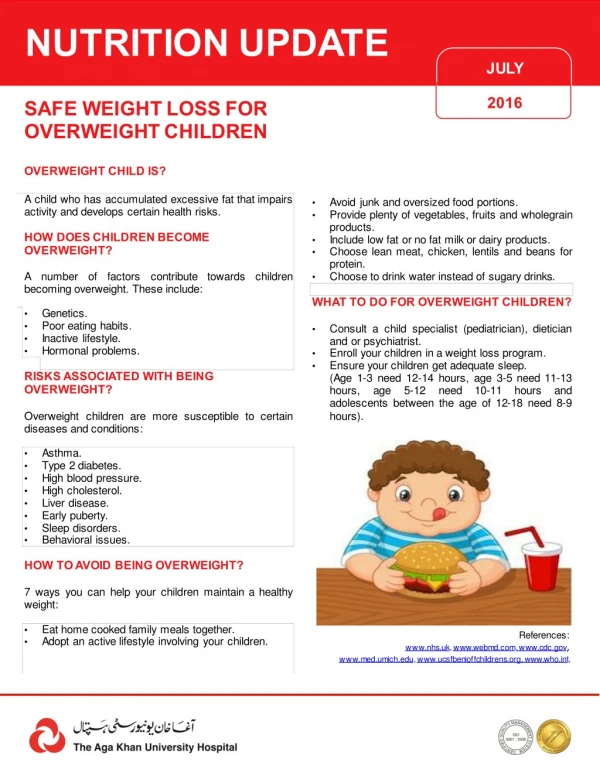
Adverse Health Consequences • Obesity increases the likelihood of: • type 2 diabetes (majority are obesity-related) • cardiovascular diseases (CHD, MI, and stroke) • several types of cancer • gallbladder disease • sleep apnea • osteoarthritis • perhaps others (e.g., Alzheimer's, depression, back pain) • Responsible for a bunch of deaths each year
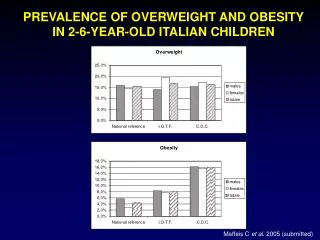
Obesity and Mortality Risk 2.5 2.0 MortalityRatio 1.5 1.0 VeryLow VeryHigh Low Moderate High 0 MenWomen 20 25 30 35 40 BMI
Etiology of Obesity Energy Expenditure Sedentary lifestyle Energy Intake High fat, high-calorie diet GeneticPredisposition
Causes: • Dietary factors • Psychosocial stressors • Genetic Factors • behavioral factors • Exercise style • Culture • Disorders/ endocrine/
Etiologic considerations for overweight children and adolescents • Endocrine disorders: • Cushing syndrome • Hypothyroidism • Pseudo hyperparathyroidism • Type2 diabetes • Genetic syndromes • Prader- Willi syndrome • Bardet-Biedel syndrome • Cohen syndrome • Central Nervous system disorders • Hypothalamic tumor • Trauma • Inflammation • Miscellaneous • Drug-induced (e.g., resperidone, tricyclic, antidepressants) • Bring eating disorder • Bulimia nervosa
The Fat Cell Is a Veritable Endocrine Factory Adiponectin Resistin Leptin Angiotensinogen Fat Cell IL-6 Stored Triglycerides Cortisol TNF-Alfa • Fat cells are continually absorbing or releasing substances in response to the body’s energy needs • Fat cells are better adapted to preserving calories than shedding them
Obesity Genetics • Environmental factors play a significant role in the development of obesity • Genetic influence on adipose tissue accumulation and distribution • More than 300 genes, markers and chromosomal regions have been associated or linked with human obesity
ارزیابی بالینی چاقی: • ارزیابی چاقی را می توان به چند روش انجام داد. • بایداز روشی استفاده کرد که ارزان –ساده- دقیق و قدرت اندازه گیری توده چربی بدن را داشته باشد. • آنتروپومتری (اندازه گیری قد و وزن و دور کمر و استفاده از BMI) ) در مطالعات اپیدمیولوژیک و ارزیابی بالینی برای بر آورد میزان چربی بدن و نحوه توزیع آن استفاده می شود که روش ساده و سریعی است.
ENERGY IN ENERGY OUT BODY MASS Genetic predisposition to store fat
Definition of Obesity Adults • Body Mass Index (BMI) = • weight (kg) • height (m) 2 • Overweight: BMI> 25 kg/m2 • Obesity: BMI> 30 kg/m2
طبقهبندي نمايه توده بدني طبيعي و غيرطبيعي
اندازه دور كمر وجود چربي در شكم كه با چربي تمام بدن غيرمتناسب باشد، يك پيشبيني كننده مستقل براي عوامل خطر و عوارض است. اندازه دور كمر با ميزان چربي شكم ارتباط مستقيم دارد و شاخص قابل قبولي براي ارزيابي ميزان چربي شكم بيمار قبل و هنگام درمان براي كاهش وزن ميباشد. افزايش دور كمر در مردان بيش از 102(94) سانتيمتر و در زنان بيش از 88(80) سانتيمتر غيرطبيعي است. اين مقادير براي كساني كه 35≥BMI دارند، استفاده نميشود.
International cut-off points for body mass index for overweight and obesity by sex between 2 and 18 years Body mass index 30kg m-2 Body mass index 25 kg m-2 Age( years) Source: Cole et al. BMJ2000; 320: 1240
گرفتن شرح: • شرح حال دوران حاملگی، وزن هنگام تولد و دیابت مادر • شرح حال اوایل تولداز نظروضعیت رشد و تغذیه • شرح حال وزنی : زمان شروع اضافه وزن و چاقی- طول مدت آن. • اثر چاقی روی زندگی فرد و خانواده • شرح حال تغذیه :شامل الگوی تغذیه معمول-مصرف غذای های فوری-میان وعده ها-عادات خاص غذایی تعداد وعده های غذائی، نوع و مقدار هر وعده غذا
شرح حال شیوه زندگی: • شرح حال میزان فعالیت جسمی روزانه شامل فعالیتهای مفید و موثر از نظر شرکت در ورزشهای انفرادی و با برنامه و سازمان یافته • نحوه استفاده از وسائل حمل و نقل • عادات غذائی ،محل غذاخوردن ، میان وعده • Sedentary behaviors- مدت زمانی که حسب عادت به مشاهده تلویزیون –کار با کامپیوتر و بازیهای کامپیوتری روزانه می پردازد
معاینه فیزیکی: • ارزیابی عمومی از نظر نحوه توزیع چربی در بدن و تظاهرات سندرومیک • اندازه گیری قد-وزن-دورکمر-فشار خون • اندازه گیری ضخامت چین • فشار خون • معاینه گردن ازنظر بزرگی تیروئید –آکانتوزیس نگریکانس • معاینه ته چشم • ارزیابی بلوغ جنسی • معاینه پوست از نظر Stria وآکانتوزیس نگریکانس • ارزیابی وضعیت تنفس از نظر آسم –آپنه تنفسی-خورخور کردن درخواب – • معاینه اندامها از نظر عوارض اورتوپدیک • معاینه شکم از نظر اندازه کبد چون خطرsteato hepatitis وجود دارد که منجر به بزرگی کبد می شود.
شرح حال عوارض چاقی • وجود آپنه تنفسی و اختلال در خواب • سابقه اختلال آندوکرین- فشار خون –دیس لپدمی-دیابت تایپ2 و ... • اثرات روان شناختی چاقی مثل آزار رساندن و مسخره کردن دیگران
Family's weight and metabolic history • BMI or BMI percentile for first- degree relatives • Relative weights of other family members • Family history, including obesity, types 2 diabetes, cardiovascular and cerebrovascular disease or obstructive sleep apnoea
MEDICAL ASSESSMENT • Obesity can be seen in association with a wide variety of genetic and endocrine disorders , the signs and symptoms of which include: • hypogonadism, • short stature, • dysmorphic features, • mental retardation • The first step in the assessment of an overweight child is a careful evaluation to identify any underlying syndromes or secondary complications.
Children with endogenous obesity are short and often have a delayed or normal bone age. • Conversely, children with idiopathic or exogenous obesity are taller and often have growth acceleration along with advancement in bone age. • A careful history and physical examination are usually adequate to rule out or suspect an endogenous cause for obesity in most children.
ارزیابی پاراکلینیک: • کلسترول، HDL و LDL، تری گلسیرید، قند خون ناشتا،آزمونهای کارکرد کبد ،کلیه ودر کودکان با کوتاه قدی،جنس مونث یا با سابقه فامیلی بیماری تیروئید ،تستهای کارکرد تیروئید انجام می شود. • گلوکز ناشتا کمتر از 110- انسولین کمتر از 15 MU درلیترهموگلوبینA1c کمتر از6/. درصد AST کمتر از 46 ALT کمتر از35 توتال کلسترول کمتراز 170 و LDL کمتر از 110،HDL کمتر از 35،تری گلسیریددرسن15-2 سال کمتر از 100و19-15 سال کمتر از 125 میلی گرم دو دسی لیترنرمال است .
Practical algorithm for diagnosing childhood and adolescent obesity
Assessment and management of the obese child or adolescent Normal weight BMI < 85th percentile Encourage healthy eating and regular physical activity Measure BMI and compare with percentile charts of BMI- for- age Overweight or obese BMI>85th percentile: Overweight BMI>95th percentile: obese • Assess for risk factors • Very obese • Abnormal physical examination • Adverse eating and exercise behavior • Family history of obesity-related disease • Devise treatment strategy with patient and family • Use one or more conventional weight- management strategies • If risk factor present • Consider investigation and referral • May benefit from non- conventional weight management strategy in specialist setting
Increase physical activity • Incidental activity • Lifestyle activity • Exercise programs • Active transport (walking, cycling)
Dietary change • Avoid severe food restriction • Reduce energy intake • Reduce portion size • Select foods with lower fat content and low glycaemic index • Increase vegetable and fruit intake • Reduce high- sugar foods and drinks • Use water as the main beveragez
Decreased sedentary behavior • Reduce time spent watching television, playing computer games, using other electronic media • Encourage alternatives to motorized transport
Community- Based prevention programs • School-based prevention programs • Classroom curriculum intervention • School food service intervention • Physical education intervention
Treatment • The approach to therapy and aggressiveness of treatment should be based on risk factors, including: • Age • Severity of obesity and morbidities • Family history and support • Primary goal for all children with uncomplicated overweight is to achieve healthy eating and activity pattern • For children with secondary complication, improvement of complication is an important goal
TREATMENT……… • DRUGS (FDA approved over 16 years) • SIBUTRAMINE Inhibition of serotonin and noradrenalin reuptake side effects: dry mouth, constipation, insomnia • ORLISTAT Selective inhibitor of pancreatic lipase Side effects: Fecal fat loss, Decrease in fat soluble vitamins