Download
1 / 1
10 likes | 215 Views
Ealing Hospital NHS Trust Outcomes of Pregnancy of Unknown Location Linda Farahani , Aikaterini Iatropoulou, Charity Khoo, Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom. INTRODUCTION

E N D
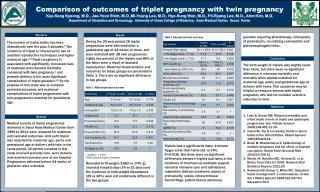
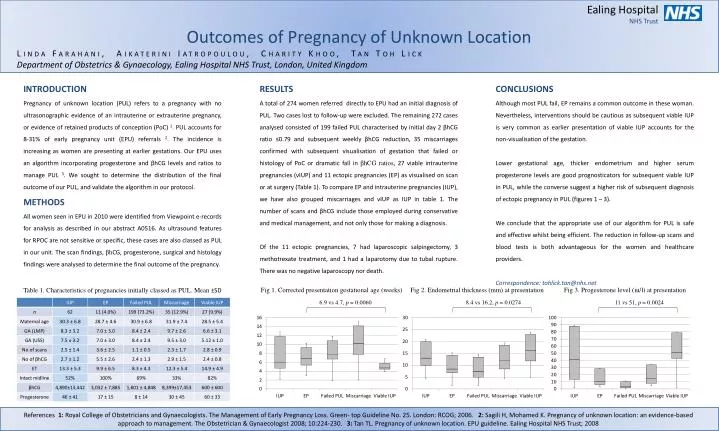
Ealing Hospital NHS Trust Outcomes of Pregnancy of Unknown Location Linda Farahani, Aikaterini Iatropoulou, Charity Khoo, Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom INTRODUCTION Pregnancy of unknown location (PUL) refers to a pregnancy with no ultrasonographic evidence of an intrauterine or extrauterine pregnancy, or evidence of retained products of conception (PoC) 1. PUL accounts for 8-31% of early pregnancy unit (EPU) referrals 2. The incidence is increasing as women are presenting at earlier gestations. Our EPU uses an algorithm incorporating progesterone and βhCG levels and ratios to manage PUL 3. We sought to determine the distribution of the final outcome of our PUL, and validate the algorithm in our protocol. METHODS All women seen in EPU in 2010 were identified from Viewpoint e-records for analysis as described in our abstract A0516. As ultrasound features for RPOC are not sensitive or specific, these cases are also classed as PUL in our unit. The scan findings, βhCG, progesterone, surgical and histology findings were analysed to determine the final outcome of the pregnancy. Table 1. Characteristics of pregnancies initially classed as PUL. Mean ±SD RESULTS A total of 274 women referred directly to EPU had an initial diagnosis of PUL. Two cases lost to follow-up were excluded. The remaining 272 cases analysed consisted of 199 failed PUL characterised by initial day 2 βhCG ratio ≤0.79 and subsequent weekly βhCG reduction, 35 miscarriages confirmed with subsequent visualisation of gestation that failed or histology of PoC or dramatic fall in βhCG ratios, 27 viable intrauterine pregnancies (vIUP) and 11 ectopic pregnancies (EP) as visualised on scan or at surgery (Table 1). To compare EP and intrauterine pregnancies (IUP), we have also grouped miscarriages and vIUP as IUP in table 1. The number of scans and βhCG include those employed during conservative and medical management, and not only those for making a diagnosis. Of the 11 ectopic pregnancies, 7 had laparoscopic salpingectomy, 3 methotrexate treatment, and 1 had a laparotomy due to tubal rupture. There was no negative laparoscopy nor death. CONCLUSIONS Although most PUL fail, EP remains a common outcome in these woman. Nevertheless, interventions should be cautious as subsequent viable IUP is very common as earlier presentation of viable IUP accounts for the non-visualisation of the gestation. Lower gestational age, thicker endometrium and higher serum progesterone levels are good prognosticators for subsequent viable IUP in PUL, while the converse suggest a higher risk of subsequent diagnosis of ectopic pregnancy in PUL (figures 1 – 3). We conclude that the appropriate use of our algorithm for PUL is safe and effective whilst being efficient. The reduction in follow-up scans and blood tests is both advantageous for the women and healthcare providers. Correspondence: tohlick.tan@nhs.net Fig 1. Corrected presentation gestational age (weeks) Fig 2. Endometrial thickness (mm) at presentation Fig 3. Progesterone level (iu/l) at presentation 6.9 vs 4.7, p = 0.0060 8.4 vs 16.2, p = 0.0274 11 vs 51, p = 0.0024 References 1: Royal College of Obstetricians and Gynaecologists. The Management of Early Pregnancy Loss. Green- top Guideline No. 25. London: RCOG; 2006. 2:Sagili H, Mohamed K. Pregnancy of unknown location: an evidence-based approach to management. The Obstetrician & Gynaecologist 2008; 10:224-230. 3: Tan TL. Pregnancy of unknown location. EPU guideline. Ealing Hospital NHS Trust; 2008