Understanding Hypothyroidism: Causes, Symptoms, and Implications for Health
580 likes | 759 Views
Hypothyroidism is a deficiency in thyroid hormones leading to a generalized slowing of metabolic processes. It's the most common endocrine disease, with a prevalence of 8:1 in females compared to males. Most cases (90%) are primary hypothyroidism, often underdiagnosed. Symptoms can include menstrual irregularities, weight gain, lethargy, and more. Subclinical hypothyroidism affects about 5% of the population, with increased detection necessary, especially in older adults and during pregnancy. This guide details its epidemiology, etiology, manifestations, and associated health burdens.

Understanding Hypothyroidism: Causes, Symptoms, and Implications for Health
E N D
Presentation Transcript
Hypothyroidism Hasan AYDIN, MD Yeditepe University Medical Faculty Endocrinology and Metabolism
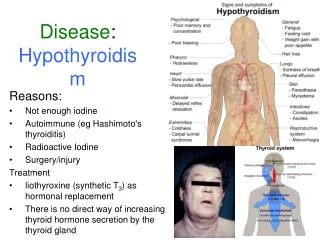
Definition A deficiency of thyroid hormones, which in turn results in a generalized slowing down of metabolic processes.
Epidemiology Most common endocrine disease Females > Males – 8 : 1 Presentation Often unsuspected and grossly under diagnosed 90 % of the cases are Primary Hypothyroidism Menstrual irregularities, miscarriages, growth retard. Vague pains, anaemia, lethargy, gain in weight In clear cut cases - typical signs and symptoms Hypothyroidism
Disease Burden • 5% of the general population are “Subclinically Hypothyroid” • 15 % of all women > 65 yrs. are hypothyroid • Detecting sub-clinical hypothyroidism in pregnancy is highly essential • All persons aged above 60 years – Order for TSH
Causes of Hypothyroidism Primary Congenital Acquired Transient Secondary Pituitary Hypothalamic
Congenital Hypothyroidism Athyreosis Dyshormonogenesis Sodium/iodide symporter mutations TPO mutations Thyroglobulin gene mutations Deiodinase defects Thyroid hormone resistance TSH-receptor defect
Acquired Hypothyroidism Iodine deficiency Autoimmune thyroid disease Hashimoto’s , Graves disease Iatrogenic Post-thyroidectomy Radioactive iodine treatment Thyroid irradiation Medications/goitrogens
Hashimoto’s Disease Struma lymphomatosa : firm, enlarged thyroid Antibodies to thyroid antigens (TPO, Thyroglobulin, TSH receptor, T4, T3) Cellular abnormalities (increased CD8+ T cells,aberrant HLA-DR expression,increased NK/K cells and cytokines) Slowly progressive disease (10 % hypothyroid) Associated with other autoimmune disease
Transient Hypothyroidism Subacute thyroiditis (de Quervain’s) Silent thyroiditis Post-partum thyroiditis (Hashimoto’s) Transient neonatal hypothyroidism
Secondary Hypothyroidism Pituitary Tumor Infectious disease Infiltrating disease Vascular insufficiency Empty sella syndrome Iatrogenic Hypothalamic Tumor Infectious disease Infiltrating disease TRH deficiency Iatrogenic
Skin and Appendages Myxedema (hyaluronic acid accumulation) Pale, cool and dry skin, hypercarotenemia Tongue is enlarged Thickened laryngeal/pharyngeal mucous membranes Slow wound healing, bruising Dry, brittle hair Temporal loss of eyebrows Brittle nails
Cardiovascular System Decreased cardiac output (stroke volume + heart rate) Increased peripheral vascular resistance Narrow pulse pressure Pericardial effusion, dilated myocardium Coronary atherosclerosis (HT,HL) ECG changes (bradycardia, low amplitude QRS, prolonged PR, ST alterations)
Respiratory System Pleural effusions Decreased ventilatory drive (hypercapnia, hypoxemia) Involvement of respiratory muscles Obstructive sleep apnea
Gastrointestinal Delayed peristalsis, distension, constipation Ascitis (rare) Achlorhydria and pernicious anemia Reduced appetite
Musculoskletal Delayed, abnormal epiphyseal ossification Impaired linear growth (short limbs) and bone age Myalgias (inflamation, infiltration) Joint effusions
Neuropsychiatric Decreased cerebral perfusion, myelination, and cortical development- retardation Slow speech, lack of concentration and memory, depression, paranoia Delay in the relaxation phase of DTR Delayed nerve conduction, carpal tunnel syndrome Perceptive hearing loss (Pendred Synd.)
Reproductive System Delayed puberty Oligomenorrhea and menorrhagia Reduced fertility Oligospermia and erectile dysfunction Hyperprolactinemia
Other Decreased erythropoetin (anemia) Decreased Factor 8 and 9 Low basal metabolic rate Increased cholesterol, TG, LDL and decreased HDL
Infantile Hypothyroidism (Cretinism) Retardation of mental development and growth Protuberant abdomen,umblical hernia, dry skin, poor hair and nail growth, delayed teeth eruption, waddling gait Epiphysial dysgenesis
Myxedema Coma Severe myxedema, bradycardia, hypotension, subnormal temperature,seizures Alveolar hypoventilation, dilutional hyponatremia are common Exposure to cold, infection, trauma, central nervous system depressants trigger coma
Solid Oedema Xanthomata
Laboratory Tests TSH T3 and T4 Thyroid antibodies RAIU Serum lipids CK, SGOT, LDH Hemogram
Differential Diagnosis Elderly patients Chronic renal failure Nephrotic states Pernicious anemia Euthyroid Sick Syndrome Down Syndrome
Co-morbidity Hypercholesterolemia Depression Infertility – Menstrual Irregularities Diabetes mellitus
Hypothyroidism and Hypercholesterolemia 14% of patients with elevated cholesterol have hypothyroidism Approximately 90% of patients with overt hypothyroidism have increased cholesterol and / or triglycerides
Lipids in Patient with Hypothyroidism Hypercholesterolemia(>200 mg/dL) Hypertriglyceridemia(>150 mg/dL) Hypercholesterolemia and mild Hyper TG Normal Lipids N= 268
LDL-C Levels Increase With Increasing Hypothyroidism Grade 246 191 168 144 137 133 LDL-C(mg/dL 1 2 3 4* 5† C Hypothyroidism Grade Basal TSH (mU/L) 1.1 3.0 8.6 22.7 44.4 63.7
Hypothyroidism and Depression Depressive symptoms are common in hypothyroidism Many hypothyroid patients fulfill DSM-IV criteria for a depressive disorder Depressed patients may be more likely than normal individuals to be hypothyroid All depressed patients should be evaluated for thyroid dysfunction
Hypothyroidism and Depression Depression Hypothyroidism Constipation Decreased Conc. Decreased libido Depressed mood Diminished interest Weight increase Fatigue Bradycardia Cardiac and lipid Abnormalities Cold intolerance Hair and skin changes Delayed reflexes Goiter Sleep decreaseSuicidal ideation Weight change Delusions
Hypothyroidism and Infertility Hypothyroidism associated with infertility, miscarriage, stillbirth 2.Infertility : Evaluate thyroid function, treathypothyroidism 3. Equivocal results: Begin therapy; discontinueif no pregnancy for several months.
Suspect Hypothyroidism Amenorrhea Oligomenorrhea Menorrhogia Galactorrhea Premature ovarian failure Infertility Decreased libido Precocious / delayed puberty
Hypothyroidism and Diabetes Approximately 10% of patients with type 1 diabetes mellitus developsub-clinical hypothyroidism In diabetic patients - examine for goitre TSH measurement at regular intervals
Many Causes, One Treatment Goal : Normalize TSH level regardless of cause of hypothyroidism Treatment : Once daily dosing with Levothyroxine sodium (1.6µg/kg/day) Monitor TSH levels at 6 to 8 weeks, after initiation of therapy or dosage change
Treatment of choice is levothyroxin Branded thyroxine recommended Brand consistency recommended No divided doses - illogical Not recommended for use : Desiccated thyroid extract Combination of thyroid hormones T3replacement except in Myxedema coma Many Causes, One Treatment
Age (in elderly start with half dose) Severity and duration of hypothyroidism (↑ dose) Weight (0.5µg/kg/day ↑ upto 3.0µg/kg/day) Malabsorption (requires ↑ dose) Concomitant drug therapy (only on empty stomach) Pregnancy ( 25% ↑ in dose), safe in lactating mother Presence of cardiac disease (start alt. day Rx) Dosage Adjustments
Starting dose for healthy patients < 50 years at 1.0 µg/kg/day Starting dose for healthy patients > 50 years should be < 0,50 µg/day. Dose ↑ by 25 µg, if needed, at 6 to 8 weeks intervals. Starting dose for patients with heart disease should be 12.5 to 25 µg/day and increase by 12.5 to 25 µg/day, if needed, at 6 to 8 weeks intervals Start Low and Go Slow
How the Patient Improves • Feels better in 2 – 3 weeks • Reduction in weight is the first improvement • Facial puffiness then starts coming down • Skin changes, hair changes take long time to regress • TSH starts showing decrements from the high values • TSH returns to normal eventually
Reduced Absorption Cholestyramine resin Sucralfate Ferrous sulfate Soybean formula Aluminum hydroxide Colestipol hydrochloride Drug Interactions Drugs that affectmetabolism • Rifampin • Carbamazepine • Phenytoin • Phenobarbitol • Amiodarone
Over-replacement risks Reduced bone density / osteoporosis Tachycardia, arrhythmia. atrial fibrillation In elderly or patients with heart disease, angina, arrhythmia, or myocardial infarction Under-replacement risks Continued hypothyroid state Long-term end-organ effects of hypothyroidism Increased risk of hyperlipidemia Inappropriate Dosage