Download
1 / 55
580 likes | 1.5k Views
Benign Conditions of the Ovaries and Fallopian Tubes Prepared by: Mr’s Raheegeh Awni 25/10/2010. FUNCTIONAL AND BENIGN OVARIAN TUMORS. The human ovary has an opportunity to develop a wide variety of tumors, the majority of which are benign.

E N D
Benign Conditions of the Ovaries and Fallopian Tubes Prepared by: Mr’s Raheegeh Awni25/10/2010
FUNCTIONAL AND BENIGN OVARIAN TUMORS • The human ovary has an opportunity to develop a wide variety of tumors, the majority of which are benign. • Ovarian tumors may be functional, inflammatory, metaplastic, or neoplastic. • During the childbearing years, 70% of noninflammatory ovarian tumors are functional.
The remainder is either neoplastic (20%) or endometriomas (10%). • The management of ovarian tumors, whether functional, benign, or malignant, involves difficult decisions that may affect a woman's hormonal status or fertility.
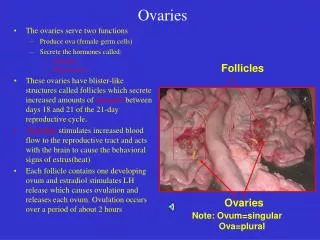
1- Functional Ovarian Cysts and Tumors • Dozens of ovarian follicles form each cycle. • to be classified a "functional cyst," the mass must reach a diameter of at least 3 cm. • Functional cysts may cause pelvic pain, a dull sensation, or heaviness in the pelvis. • If the ovarian follicle fails to rupture in the course of follicular development and ovulation, a A- follicular cyst, lined by one or more layers of granulosa cells, may develop.
B- a lutein cyst may develop if the corpus luteum becomes cystic, grows to over 3 cm, and fails to regress normally after 14 days. • Hemorrhagic cysts, especially hemorrhagic corpus luteum cysts, are more likely to cause symptoms and are more vulnerable to rupture toward the end of the menstrual cycle.
The calutein cysts: Other specific types of lutein cysts that may develop in association with the high levels of hCG present in patients with a hydatidiform mole or choriocarcinoma. • theca-lutein cyst a cyst of the ovary in which the cystic cavity is lined with theca interna cells. • Patients undergoing ovulation induction with gonadotropins or clomiphene may also develop the calutein cysts. • The calutein cysts are usually bilateral, may become quite large (>30 cm), and characteristically regress slowly after the gonadotropin level falls. • Can cause massive ascites and dangerous problems with systemic fluid imbalance.
A luteoma of pregnancy is a related condition in which there is a hyperplasic reaction of ovarian theca cells, presumably from prolonged hCG stimulation during pregnancy. • The luteomas characteristically appear as brown to reddish-brown nodules that may be cystic or solid. • A luteoma of pregnancy may be associated with multifetal pregnancies or hydramnios.
They can cause maternal virilization in 30% of women and, less often, ambiguous genitalia in a female fetus. • Although ovarian enlargement may be impressive, surgical resection is not indicated, because luteomas regress spontaneously postpartum.
C- Polycystic ovarian syndrome, a functional disorder generally associated with chronic anovulation and hyperandrogenism, can also produce enlarged ovaries with multiple simple follicles.
Clinical features • An ovarian follicular cyst: • asymptomatic, • unilocular ("simple"), • can reach 15 cm in diameter. • regresses during the subsequent menstrual cycles.
A lutein cyst: • smaller but more firm • solid in consistency • more likely to cause pain or signs of peritoneal irritation. • Because it may continue to produce progesterone, it is also more likely to cause delayed menses. • a functional ovarian cyst may undergo torsion (or may rupture, which may produce acute lower abdominal pain and tenderness and significant hemoperitoneum.
Diagnosis. • a 5 to 8-cm cystic adnexal mass is noted on bimanual examination; • it is confirmed when the lesion regresses over the course of the next several cycles. • mobile, • unilateral, • not associated with ascites.
the mass may exceed 8 cm and be quite tender to palpation. • On occasion, hemorrhagic lutein cysts may have a solid rather than a cystic consistency. • A pelvic ultrasound
If the patient has delayed menses, abnormal uterine bleeding, or severe pelvic pain, the differential diagnosis must include: • ectopic pregnancy, • pelvic abscess, • or adnexal torsion of a neoplastic cyst. A pregnancy test (hCG), diagnostic laparoscopy, or laparotomy may be needed
Management. • When a reproductive-age patient who is asymptomatic or experiencing only mild symptoms presents with an adnexal cyst that is less than 6 cm in diameter, wait and reexamine the patient after her next menses. • Treatment with hormones (usually low-dose contraceptive agents) to suppress gonadotropin levels and to prevent development of another cyst • If the cystic mass is between 6 and 8 cm, or if it is fixed or feels solid, a pelvic ultrasound study should be obtained to determine that it is unilocular. • Laparoscopic cystectomy to differentiate between a functional and a neoplastic ovarian cyst.
2-Benign Neoplastic Ovarian Tumors • neoplasms may be divided generally by cell type of origin into three main groups: • Three basic types of ovarian tumors exist, They include: • Epithelial tumors: they develop in the epithelium, the thin layer of tissue that covers the ovaries. • Germ cell tumors: they occur in the egg-producing cells • Stromal cell tumors: they develop in the estrogen & progesterone – producing cells.
Type of Ovarian NeoplasmNo • Benign cystic teratoma • Serouscystadenoma/cystadenofibroma • Mucinouscystadenoma/cystadenofibroma • Fibroma • Serous carcinoma • Endometrioid carcinoma • Mixed carcinoma • Serous borderline tumor • Brenner tumor, • Thecoma • Clear cell carcinoma • Mucinous carcinoma • Mucinous borderline tumor • Immature teratoma • OTHERTS
A- Epithelial ovarian neoplasms. • These tumors are believed to be derived from the mesothelial cells lining the peritoneal cavity and also lining the surface of the ovary in greater density. • Similar tumors occasionally arise from the mesothelial lining of the pleural cavity. • The most common epithelial ovarian tumors retain their serous cell type and are termed serous cystadenomas.
bilateral • Of all serous tumors, about 70% are benign, 5% to 10% have borderline malignant potential and 20% to 25% are malignant, depending largely on the patient's age. • tend to be multilocular,. • Histologically, serous tumors characteristically form psammoma bodies (sand), which are calcific, concentric concretions. • Psammoma bodies occur occasionally in benign serous neoplasms and frequently in serous cystadenocarcinomas. • Papillary patterns
The mucinous neoplasms: • huge size, • often filling the entire pelvis and abdomen. • multilocular, • and benign mucinous tumors are bilateral in less than 10% of cases. • About 85% of mucinous tumors are benign. Mucinous tumors are often associated with appendix.
The Brenner tumor: • is a small, • smooth solid ovarian neoplasm, • usually benign, • with a large fibrotic component that encases epithelioid cells that resemble transitional cells of the bladder • In about 33% of cases, Brenner tumors are associated with mucinous epithelial elements.
3- Sex cord-stromal ovarian neoplasms • Sex cord-gonadal stromal tumour (or sex cord-stromal tumour) is a group of tumours of sex cord-derived from tissues of the ovary and testis. • These tumors include fibromas, granulosa-theca cell tumors, and Sertoli-Leydig cell tumors. • Combinations of the latter two types are termed gynandroblastomas
The tumors in this category derive from the sex cords and specialized stroma of the developing gonad. • The embryologic origins of granulosa and theca cells as well as their counterparts in the testes, the Sertoli and Leydig cells, arise from cells that make up this specialized gonadal stroma.
Tumour types in order of prevalence • 1- Granulosa cell tumour. • This tumour produces granulosa cells, which normally are found in the ovary. • It is malignant in 20% of women diagnosed with it. • It tends to be present in women in the 50-55yo age group with post menopausal vaginal bleeding.
Uncommonly, a similar but possibly distinct tumour, juvenile granulosa cell tumour, presents in pre-pubertal girls with precocious puberty. • In both groups, the vaginal bleeding is due to oestrogen secreted by the tumour. • In older women, treatment is total abdominal hysterectomy and removal of both ovaries. • In young girls, fertility sparing treatment is the mainstay for non-metastatic disease.
2- Sertoli cell tumour. This tumour produces Sertoli cells, which normally are found in the testicle. • This tumour occurs in both men and women.
3- Thecoma. This tumour produces theca of follicle, a tissue normally found in the ovarian follicle. • The tumour is almost exclusively benign and unilateral. • It typically secretes androgens, and as a result women with this tumour often present with new onset of hirsutism or virilisation
4- Leydig cell tumour. This tumour produces Leydig cells, which normally are found in the testicle and tend to secrete androgens. • 5- Sertoli-Leydig cell tumour. This tumour produces both Sertoli and Leydig cells.
6- Gynandroblastoma. • A very rare tumour producing both ovarian (granulosa and/or theca) and testicular (Sertoli and/or Leydig) cells or tissues. • Typically it consists of adult-type granulosa cells and Sertoli cells but it has been reported with juvenile-type granulosa cells
It has been reported to occur in the ovary usually, rarely in the testis. • Due to its rarity, the malignant potential of this tumour is unclear; there is one case report of late metastasis.
4- Germ-cell tumors • Germ-cell neoplasms can occur at any age. • They make up about 60% of ovarian neoplasms occurring in infants and children. • The most common ovarian neoplasm is the benign cystic teratoma, • 10 -15% of teratomas are bilateral.
The benign cystic teratoma, commonly referred to as a dermoid cyst • It is composed primarily of ectodermal tissue (such as sweat and sebaceous glands, hair follicles, and teeth), • some mesodermal and rarely endodermal elements.
These are slow-growing tumors. • Half are diagnosed in women between 25 and 50 years of age. • Most are less than 10 cm in diameter. • Because of the oily secretion of the sebaceous glands, presence of hair, and the presence of a dermoid tubercle which often contains a hard, well-formed tooth,
Other tissue commonly found in benign cystic teratomas include mature brain, bronchus, thyroid, cartilage, intestine, bone, and carcinoid cells.
Mixed ovarian neoplasms • most common ovarian tumor in which the neoplastic elements are composed of more than one cell type is the cystadenofibroma, or the fibrocystadenoma. • These tumors generally take their characteristics from the epithelial component, although they tend to be more solid than the epithelial ovarian neoplasms.
Diagnosis of benign ovarian tumors • are asymptomatic unless they undergo torsion or hemorrhage • Bimanual pelvic examination • Pelvic ultrasonography, transvaginal ultrasonography, Doppler. • A pelvic ultrasound will be highly suggestive of a dermoid cyst, especially if it is found to include a tooth-like calcification
Tumor markers, such as serum CA 125, may help to distinguish between benign and malignant masses • Laparoscopy is helpful in distinguishing between a uterine myoma, and an ovarian tumor,
Management of Ovarian Neoplasms • No persistent ovarian neoplasm should be assumed to be benign until proven so by surgical exploration and pathological examination • Exploratory laparotomy • A scitic fluid should be collected on opening the peritoneal cavity and sent for cytologic examination. • Unilateral salpingo-oophorectomy.
appendectomy is also indicated in such patients • If the patient is young and nulliparous, the ovarian neoplasm is unilocular, an ovarian cystectomy with preservation of the ovary may be performed. • In an older woman, a total abdominal hysterectomy and bilateral salpingo-oophorectomy (TAH-BSO)
Cystic teratomas ("dermoids") • RX. ovarian cystectomy. • In a patient with a gonadoblastoma, dysgenetic ovaries are usually present, necessitating bilateral salpingo-oophorectomy • With the possibility of embryo transfer, the uterus should be left in situ if future fertility is desired, even when both ovaries have been removed.
Most benign tumors of the fallopian tubes are infectious/inflammatory (hydrosalpinx) • Benign neoplasms of the oviducts are rare. • Although the tubes, uterine corpus, and uterine cervix are from the same (primordial tissue), the tubes have less of a tendency toward neoplastic transformation
Tubal neoplasms that do occur are epithelial adenomas and polyps, myomas from the tubal musculature, cysts from the mesothelium, or angiomas from the tubal vasculature.